Download
1 / 50
660 likes | 1.73k Vues
Evaluation and Interpretation of Renal Function. Dr . Shikha Rao. University College of Medical Science & GTB Hospital, Delhi. Functions of Kidney. Regulation of fluid and electrolyte balance by adjusting volume of water lost in urine renin and angitensin system

E N D
Evaluation and Interpretation of Renal Function Dr. ShikhaRao University College of Medical Science & GTB Hospital, Delhi
Functions of Kidney • Regulation of fluid and electrolyte balance by • adjusting volume of water lost in urine • renin and angitensin system • Regulate plasma ion concentrations: • sodium, potassium, and chloride ions (by controlling quantities lost in urine) • calcium ion levels (through synthesis of calcitriol) • Regulation of acid-base balance • by controlling loss of hydrogen ions and bicarbonate ions in urine
Excretion of waste products of protein metabolism –urea, creatinine. • Endocrine functions • renin, Erythropoeitin, • 1,25 dihydroxycholecalciferol- conversion only in kidney
Why evaluating renal function is important • To detect possible renal damage and assessment of its severity • To diagnose renal disease • To observe the progress of renal disease • To monitor the safe and effective use of drugs which are excreted in the urine
Evaluation of renal function • Clinical markers of renal function • urine output • BUN • S.Creatinine • Assessment of GFR • S. Creatinine based nomograms • Renal clearance techniques
Tubular function tests • urinary concentrating ability • urine to plasma osmolar ratio • free water clearance • urine to plasma creatine ratio • sodium and urea conservation • indices of tubular injury • Renal hemodynamics measurement • renal plasma flow and RBF
Urine output • Perioperative oliguria <0.5 ml/kg/hr • Prerenal response to intravascular hypovolemia or a physiologic response to surgical stress • Complete / abrupt cessation – postrenal obstruction • Unreliable marker of ARF • Vary from anuria to polyuria • Nonoligouric renal failure –MC manifestation of Acute kidney injury
Blood Urea Nitrogen • Metabolism of NH3 in liver (Protein catabolism: Amino acid Ammonia (Liver) Urea (Kidney) • Urea is readily filtered at glomerulus but 40-50% is reabsorbed • Not a reliable indicator of renal function (GFR) • Normal: 8-20 mg/dL
Decrease in: starvation, liver disease (protein def) • Increase in : ↓GFR( renal disorders and urinary obstruction), ↑protein catabolism (trauma, sepsis, degradation of blood, high-protein diet)
Serum Creatinine • Reflects the balance b/w Creatinine production (M: 20-25 mg/kg, F: 15-20 mg/kg): related to muscle mass, physical activity, protein intake and catabolism & Creatinine excretion by kidney • Normal: M: 0.8 - 1.3 mg/dL, F: 0.6 - 1 mg/dL • Reliable marker of stable renal function • Inversely related to glomerular filtration rate(doubling of S.Creatinine implies a halving of GFR )
Increases: large meat meals, barbiturates, acetoacetate (ketoacidosis), Cimetidine & trimethoprim- blocks creatinine secretion by tubule • Decreases: N acetyl cysteine • GFR declines with age (5% / decade), muscle mass also declines creatinine relative normal despite decreased GFR
Cystatin C • Under Investigation • Early detection of renal dysfunction – 2nd day • Cysteine protease inhibitor • Released into circulation by nucleated cells • Completely filtered at glomerulus (not secreted) • Related to GFR & S. Creatinine • Disadv :Levels affected by immunosuppressive drugs, inflammation…
Measurement of GFR • Glomerular filtration -index of overall excretory function • Vol. of fluid filtered into Bowman’s capsule per unit time Methods • clearance of inulin, creatinine, EDTA and DTPA • S.Creatinine based nomograms
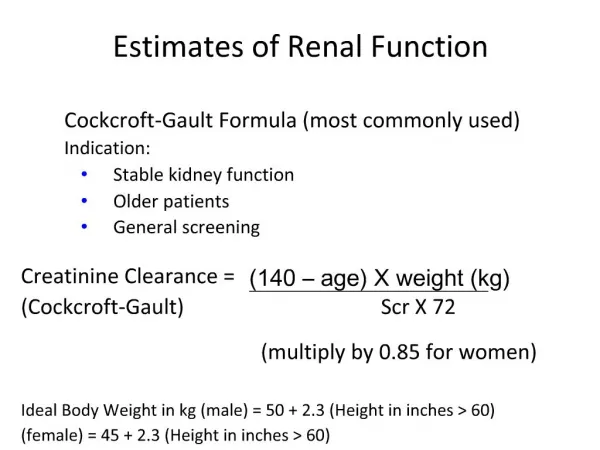
Assessment of GFR • S.Creatinine based nomograms – based on population studies • Avoid necessity of timed urine sample Eg- Cockcroft and Gault equation (GFR = Cr Cl) CrCl = (140-age) x weight (kg) x constant 72 x serum creatinine (mg/dl) • For females, value is multiplied by 0.85
Body weight may alter GFR substantially (as in obese or edematous / cachectic patients) • Modified by Robert & associates - whole body weight replaced by ideal body weight • Limitation – rapidly changing renal function
Clearance • The “clearance” of a solute is the virtual volume of blood that would be totally cleared of the solute in a given time. • Solutes come from blood entering the kidneys. • Rate at which kidneys excrete solute into urine = rate at which solute disappears from blood plasma
Principles of clearance • Some substances when filtered, enter the tubules are not reabsorbed and so100% excreted= GFR (inulin= gold standard for GFR, creatinine (but this one partially reabsorbed, particularly in uremia, then clearance<GFR • Some substances are filtered, enter tubules, and more of the substance is secreted into the tubules . Clearance>GFR • Some substances are filtered, enter tubules, but are completely reabsorbed, so they do not reach the final urine
For solute X (using Ficks eqn) Conc. of X in urine Volume of urine formed in given time Cx = Ux x V Conc. of X in systemic blood plasma Clearance Px
Solutes used to measure GFR • Required properties are: • Solute should be freely-filtered (conc. in Bowman’s space = conc in blood plasma) • Tubules do not absorb, secrete or metabolize X • Thus, amount of X in urine per unit time = that which glomerulus filters per unit time • INULIN is such a substance that satisfies all of these criteria and is commonly used to measure GFR
Inulin Clearance • Inert polyfructose sugar • Completely filtered by glomerulus • Neither secreted nor reabsorbed by renal tubule • Volume in ml of plasma cleared of inulin per minute represents GFR Measurement • After IV loading dose 30-50 mg/kg • Continuous infusion to establish steady state plasma concentration of 15-20 mg/dl • Bladder is flushed with air to eliminate any pooled urine
Carefully timed plasma and urine samples are taken • GFR: Cin = Uin x V Pin • Inulin clearance is “gold standard” for measurement of GFR • laborious and requires meticulous attention to detail, time consuming- Seldom used clinically • Normal inulin clearance • 110-140 ml/min/1.73m2 - males • 95-125 ml/min/1.73m2 - females
Creatinine clearance • Endogenous end product of creatine phosphate metabolism • simple inexpensive bedside estimate of GFR • Usually measure over 24 hr period to get reliable results samples taken before breakfast CCr = UCr x V PCr
Creatinine clearance can track changes in GFR as it alters creatinine excretion (UCr x V) • Guide alteration in renal function & prognosis – nephrotoxic drugs ( aminoglcosides, calceneurin antagonists) • When GFR very low- variability of CC is lost s/o deterirating renal function
Grouping of patients according to GFR *This term applies to patients with chronic renal failure
Limitation • Normally 20% creatinine is secreted by tubules, Creatinine clearance overestimates GFR (CC:IC = 1.2:1) • In c/o decreasing GFR, tubular secretion of creatinine increases - CC:IC = 1.8:1
Plasma Clearance • Measurement of rate of disappearance (plasma Clearance) of a substance that is completely eliminated by glomerular filtration • Involves Bolus or infusion of a Marker followed by measurement of multiple plasma levels • Markers used-Non Radio Active inulin and iothalamate, radio isotopes of EDTA & DTPA
Tubular function tests • Measure urinary concentrating ability & sodium & urea handling • Distinguish oliguria of dehydration (prerenal syndrome) from that due to tubular injury (ATN) • Prerenal- reversed by restoration of intravascular volume (except severe sepsis & hepatorenal syndrome of liver failure)
Urinary Osmolality - measures concentrating ability • Sensitive Marker • Normal : 300-900mOsm/L • Can reach maximum of 1200 mOsm/L • Pre Renal States –urine osmolality markedly increased • In ATN loss of concentrating ability l/t dilute urine with high sodium
Urine to Plasma osmolor Ratio (U: Plosm) • Normal Serum osmolality = 280-300 mOsm/kg • Pre Renal syndrome U : Plosm > 1.5 • Acute tubular necrosis U : Plosm = 1.0 (isothenuria a/w oligouria) • Isothenuria also seen in pre renal state when diuretics are administered
Free water clearance (CH2O) • Measure of Renal Water regulation by tubular dilution or concentration of urine • CH2O vary from +18 l to -8 l /day • (Hypervolemia –positive CH2O, Hypovolemia-negative CH2O) • Osmolor clearance of the solute is subtracted from urine flow rate to give free water clearance • With onset of ATN-Urine becomes isoosmolar and CH2O ~ 0 • CH2O – not provide much information
Urine to Plasma Creatinine Ratio • Represents proportion of water filtered by the glomerulus that is abstracted by entire tubule • Pre renal state increases 100 fold • Acute Tubular necrosis < 20:1
Sodium and Urea Conservation Urine Sodium • Pre Renal state • Oliguria with very low urine sodium(UNa)<20 mEq/l • Acute Renal Failure • Urine sodium exceeds 60-80 mEq/l
Fractional Excretion of Sodium • Additional means to evaluate tubular function in hyper and hypo volumia • FENa expresses sodium clearance as a percentage of creatinine clearance • In Hypovolemia, Sodium clearance and FENa is less than 1% of creatinine clearance • Tubular dysfunction increases to more than 3%
Indices of Tubular function 2microglobulin • Protein component of MHC • Normally filtered by glomerulus & undergoes partial tubular reabsorption • Distinguish glomerular & tubular injury
Glomerular injury – serum levels of 2microglobulin increase whereas urinary levels decrease used as early sign of rejection in renal transplantation • Primary tubular injury-impaired reabsorption leads to vice-versa
Urinary N Acetyl B-D-glucosaminidase (NAG) • Tubular enzyme raised insubclinical tubular injury • Uses • early detection of rejection intransplant pts • follow course of CRF therapy
Renal Plasma Flow & Renal Blood Flow-usingp- Aminihippurate clearance • There are certain substances which the kidneys completely clear from plasma during a SINGLE PASSAGE through them. • Glomerular filtration • Proximal tubular secretion • p-aminohippurate (PAH) is such a special solute.
Renal clearance of PAH = arterial renal plasma flow • Thus, PAH clearance is a good estimate of renal plasma flow • Laborious technique • Effective RPF = 660 ml/min/1.73m2 • Limitation • renal failure • surgical stress
Renal handling of PAH • PAH is an organic acid that is not usually present in the body, so given by IV infusion • Note that there is none left in the renal vein - all cleared in first pass
Filtration fraction • Fraction of RPF that is filtered at glomerulus • FF = GFR RPF • Normal = 0.2 • Represents changes in periglomerular arteriolar tone
Total renal blood flow • Flow probes – doppler technique • Thermodilution estimation of renal vein effluent • Contrast ultrasonography
References • Miller’s Anaesthesia, 7th ed. Functional anatomy and renal physiology. • Wylie and Churchill Davidson’s. Functional anatomy and renal physiology, 6th ed. • Barash Clinical Anaesthesia, Functional anatomy and renal physiology, 5th ed. • Ganong WF. Review of Medical Physiology, 20th ed.
Urinanalysis - Appearance • Blood (haematuria) • Check with Dipstix (blood, sugar, protein). • Simple, cheap, routine, easy to re-check and unlikely to make mistakes. But not quantifiable, just checks for presence. • Very concentrated – dark/smoky colour. • Very clear urine with high frequency of urination indicates it’s less likely to be a bacterial problem. • Discoloration may also be due to:(normal-pale yellow or amber) • Jaundice, haemoglobinuria. • Drugs (e.g. antibiotics). • Food (e.g. beetroot). • Disease (e.g. porphyria – Madness of King George where his urine was purple)
Drawbacks of Clearance Methods • Measuring clearance means , overall nephron function (~2 million nephrons in both kidneys) • This gives the sum of all transport processes occurring along nephrons • So, no information about precise sites and mechanisms of transport • Must therefore use studies on individual nephrons, tubule cells or cell membranes to obtain this data
Urinalysis • Routinely done for evaluating renal function • Routine urinalysis: pH, specific gravity, glucose, protein, bilirubin, urinary sediment • Specific gravity > 1.018 after overnight fast adequate renal concentrating ability