Download
1 / 35
400 likes | 1.42k Vues
Mastitis. Joe Breuner, M.D. Thanks to . Doug Trotter, who gave this talk 18 months ago. Case Presentation. Healthy 25 year-old woman, G2P2, with a 6 week-old infant Infant is fully breast-fed Patient is fatigued due to caring for 2 young children

E N D
Mastitis Joe Breuner, M.D.
Thanks to Doug Trotter, who gave this talk 18 months ago
Case Presentation • Healthy 25 year-old woman, G2P2, with a 6 week-old infant • Infant is fully breast-fed • Patient is fatigued due to caring for 2 young children • Husband is Boeing engineer, stressed because of likely upcoming layoff
Case Presentation • At 6 week visit, she reports 2 episodes of moderately painful swelling in upper inner quadrant of R breast; it occurred once in L breast • It usually resolves, but she wants to know why it happens, and what to do
Case Presentation • Exam: • Afebrile • Looks tired but otherwise well • Normal nipple and breast; no lumps or indurated areas • No skin changes or lymphadenopathy
Case Presentation • Exam: • Afebrile • Looks tired but otherwise well • Normal nipple and breast; no lumps or indurated areas • No skin changes or lymphadenopathy • Dx: Milk stasis or “plugged duct”
Milk stasis • Risk factors for milk stasis: • Fatigue, stress • Infrequent feeding • Incomplete emptying of breast • Ill-fitting bra • Pumps, shields • Prior breast trauma or infection
Milk stasis • Treatment for milk stasis: • Heat application • Massage toward nipple • Frequent, relaxed nursing • Change position to promote emptying • Avoid pumps, shields
Case Presentation • Pt calls you Sunday afternoon, 3 PM, now 7 weeks postpartum • Had recurrent swelling of upper inner quadrant R breast yesterday, but didn’t resolve • Now 2 hrs of fever, chills, increased tenderness
Case Presentation • Pt calls you Sunday afternoon, 3 PM, now 7 weeks postpartum • Had recurrent swelling of upper inner quadrant R breast yesterday, but didn’t resolve • Now 2 hrs of fever, chills, increased tenderness • Dx: Acute mastitis
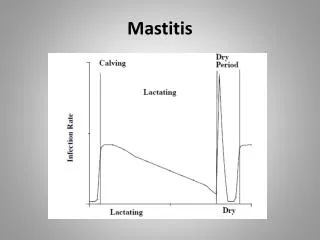
Mastitis • Incidence: 2 - 3% of lactating women
Mastitis • Incidence: 2 - 3% of lactating women • More common at 2 - 6 weeks post-partum, but can occur at any time
Mastitis • Incidence: 2 - 3% of lactating women • More common at 2 - 6 weeks post-partum, but can occur at any time • More common in primiparas, but probably due to bias
Mastitis • Incidence: 2 - 3% of lactating women • More common at 2 - 6 weeks post-partum, but can occur at any time • More common in primiparas, but probably due to bias • Risk factors: milk stasis, age > 30, stress, fatigue, professional employment of mother or father
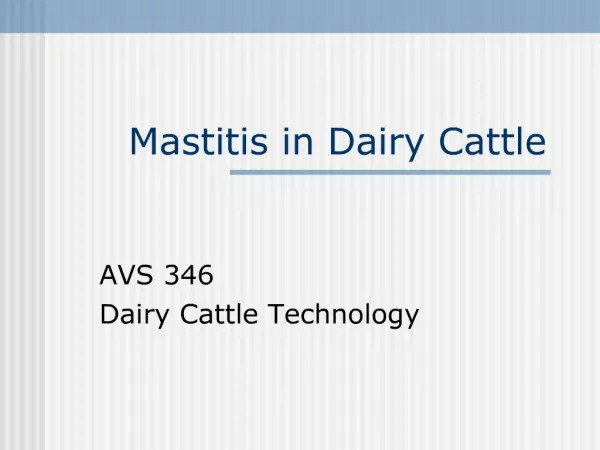
Mastitis Normal breast architecture
Mastitis • 1970 Series: • 71 cases of acute lactational mastitis • Peak incidence at 2-3 weeks postpartum • No infants weaned; none became ill • 11% developed abscesses; 75% of those required surgical drainage • Abscess more likely if antibiotics delayed • 8% developed mastitis in a later pg
Mastitis • 1975 Series: • 65 cases in 2,534 women: 2.5% incidence • Average onset 5 weeks postpartum • 14% had missed feed or rapidly weaned • 12% had nipple fissure beforehand • 74% had been nursing normally • 5% developed abscesses, all in pts who chose to wean
Mastitis • 1978 Series: • Similar results to prior studies • No abscesses if prompt antibiotic treatment and continued nursing
Mastitis • Etiology: • 50% or more: S. Aureus • Other organisms: E. Coli, S. pyogenes
Mastitis • Etiology: • 50% or more: S. Aureus • Other organisms: E. Coli, S. pyogenes • Source: infant nasopharynx (?)
Mastitis • Etiology: • 50% or more: S. Aureus • Other organisms: E. Coli, S. pyogenes • Source: infant nasopharynx (?) • Mechanism: via milk ducts or nipple fissure
Mastitis • Treatment: • Prompt antibiotics: • PO: Dicloxacillin, cephalexin, erythromycin • IV: Nafcillin, cefazolin • Continued frequent nursing • Heat application • Massage toward nipple • Antipyretics
Mastitis • In non lactating or pregnant women, consider early referral, as cancer is much more common.
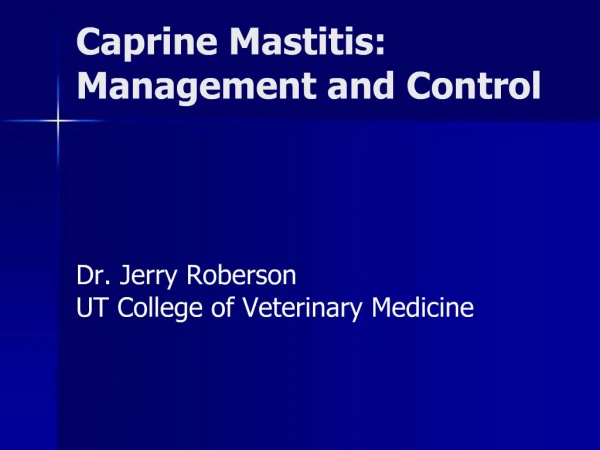
Breast Abscess Breast abscess with early skin necrosis
Breast abcess • Consider diagnosis in mastitis which fails to respond to antibiotics after 2-3d (may not feel fluctuant) • refer to breast surgeon for incisional drainage and biopsy-- • 10-15% of breast carcinomas in women<40 are found during pregnancy or lactation
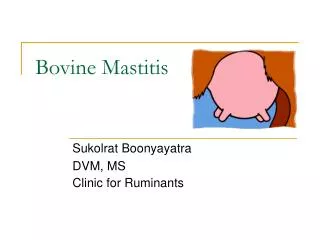
Breast Abscess Inflammatory breast cancer
Neonatal Mastitis • Occurs up to 5 weeks of age • Girls outnumber boys 2 : 1 • Etiology: 85% S. aureus, also E. coli, group D Streptococcus
Neonatal Mastitis • Occurs up to 5 weeks of age • Girls outnumber boys 2 : 1 • Etiology: 85% S. aureus, also E. coli, group D Streptococcus • Treatment: • Prompt antibiotics (IV?) • Careful needle aspiration if abscess
Candida Infection • Burning pain with nursing • Mild erythema & pruritis of nipple; findings may be subtle • Associated with thrush in the baby • May be intraductal
Candida Infection • Treat mother and baby with topical antifungals or Gentian violet • May be recurrent • If no response to topical therapy, may use oral fluconazole 150 mg qd X 5d