Download
1 / 28
280 likes | 382 Vues
Fever Without Source 1-36mo. Case 1. 5mo girl, fever, well-appearing, no underlying medical problems VS nml except T 39.8 R; exam normal Anything else you want to know? What’s your approach? What next?. Case 1 (cont.). She is incompletely immunized.

E N D
Case 1 • 5mo girl, fever, well-appearing, no underlying medical problems • VS nml except T 39.8 R; exam normal • Anything else you want to know? • What’s your approach? What next?
Case 1 (cont.) • She is incompletely immunized. • Any infant <6mo by definition since they hasven’thad 3 sets of Hib +Prevnar. Risk of bacteremia approx 5%. So… • What next? • Tests • CBC + diff • Blood culture • UA + culture • CXR
Case 1 (cont) • WBC = 15,500 /microL • Bands = 1600 / microL • UA neg • Blood culture recommended if WBC < 15,000/microL; often ordered simultaneously; can be held until WBC is back • CXR not indicated
Case 1 (cont) • Antibiotics? • YES! • Recommendation: ceftriaxone • Admit or home? • Home only if 24 hour follow up
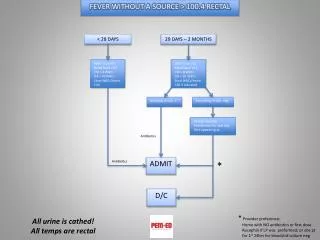
Case 1 (cont.) • Take home points: • Any child under 6mo old is by definition incompletely immunized. They haven’t received 3 doses of Hib and Prevnar. • The risk of bacteremia in incompletely immunized infants is 5% (data use from pre-Hib/Prevnar studies • All temps should be rectal, all urines cathedif not potty trained • Fever in 3-36mo is temp >39C (102.2F) • WBC >15,000/microL warrants Bcx and removes infant from low risk group • Must have follow up within 24 hrs to discharge
Case 2 • 7mo girl, fever, well-appearing, no underlying medical problems • VS nml except T 39.8 R; exam normal • Anything else you want to know? • Immunizations complete • What’s your approach? What next?
Case 2 (cont.) • Completely immunized, risk of bacteremia <1% • What next? • Test: • UA + culture
Case 2 (cont.) • UA neg • Antibiotics? • No. • Dispo? • Home with 24-48 hr follow up
Case 2 (cont.) • Take home points • In completely immunized children, risk of bacteremia is <1% • UA + culture in all girls 3-24mo with fever >39C
Case 3 • 9mo boy, well appearing, no underlying medical conditions, immunizations complete, home temp 39.5C oral • VS nml except T 38.2C • Anything else you want to know? • Circumcised? No. • Is temp rectal? No, oral. Repeat rectal T = 39.0C • Tests?
Case 3 (cont.) • UA + culture • UA shows WBC & bacteria • Treat and home with follow up
Case 3 (cont.) • Take home points • Always check immunization status • Make sure the temps are rectal • Home temps are as good as ED temps • In boys, always check for circumcision • UTI in uncircumcised boys with FUS = 10-25% • UTI in circumcised boys with FUS = 2-4% • All completely immunized children with =>39C and FUS should have UA + cxIF; 1. Uncircumcised <12mo; 2. Circumcised <6mo; 3. Girl <24 mo.
Case 4 • 2 ½ yo boy, fever for 3 days, well appearing, no med problems; immunizations complete, intake down a little • PE: VS BP 80/35, HR 143, RR 43, T 40.2C SaO2 96%; mild diffuse abd tenderness • Anything else you want to know? • Cap refill 3 sec • What’s your approach?
Case 4 (cont.) • Know age appropriate VS • T and RR are abnormal • RR > 40 = tachypnea • T > 39C = fever • What next? • Tests? • CBC + diff • Blood cultures • CXR • CRP • UA + cx
Case 4 (cont.) • WBC 23,000/microL • CXR neg • CRP 85mg/L / 8.5mg/dL • Blood culture not needed since fully immunized; bacteremia <1% • UA + culture possible but not really needed
Case 4 (cont.) • Treatment? • Yes • Amoxicillin • f/u in 24-48 hrs
Case 4 (cont.) • Take home points • 1-5yo tachypnea >40bpm • WBC > 15,000/microL suggests pyogenic infection; >20,000/microL with tachypnea, think PNA • Here CXR: 1. radiographic PNA may lag behind symptoms; 2. hypovolemic patients with PNA may have neg CXR; evident after volume repletion • Radiographic PNA found in 20-30% of febrile young children without clinical evidence of PNA, but with WBC =>20,000/microL • Studies support the use of CRP levels when considering PNA. Elevated levels suggest bacterial etiology • No blood cultures needed since fully immunized
Case 5 • 1.5mo girl, well appearing, no med probs, VS normal for age • PE: T 39.4 R, otherwise nml • Anything else you want to know? • What’s your approach?
Case 5 (cont.) • Tests • CBC + diff • Blood culture • UA + culture • CXR
Case 5 (cont.) • CBC 13,000/microL • UA neg • CXR not needed • Anything else you want to know? • Bands 4176/microL • Nml <1500/microL
Case 5 (cont) • Plan? • LP or not? • Yes • Antibiotics or not? • Yes, IM rocephin • Home vs admit? • Home OK • Since fever + high bands in 1.5mo, suggested to treat with IM rocephin and f/u in 24 hrs • Also since patient is 1-3mo and plan involves treating with antibiotic, recommendation is to do LP prior to antibiotics • 24hr f/u showed Bcx no grow, Ucx +growth
Case 5 (cont) • Take home points • Check bands… order diff’s • CXR in 1-3 mo recommended only with 1+ pulm symptom • RR >50, rales, rhonchi, retractions, wheezing, coryza, grunting, stridor, nasal flaring, cough • LP before antibiotics in this age group • LP not always necessary if caregivers knowledgeable, have transportation, well-established f/u. not recommended to give abx • UTI possible with nml UA • Recommendation for most: CBC +diff, Bcx, UA +Cx, CSF cell count +Cx; come clinicians elect to perform fewer labs. • There are no guidelines for minimal evaluation of fever in well-appearing infants age 29-60d.
Case 6 • 3mo boy, well appearing, no med probs, • PE 38.2R, otherwise VS nml • Anything else you want to know? • What is your approach?
Case 6 (cont) • Tests: • CBC + diff • UA • Blood cx • What next? • LP • In 1-3mo, <5K or >15k/microL suggests need for LP
Case 6 (cont) • WBC 15,600/microL • UA neg • Cultures pending • CSF neg • What next?
Case 6 (cont) • Treatment? • Antibiotics? • Yes, Ceftriaxone • Dispo • Admit? • Yes • WBC >15000/micoL, suggests admission with parental Abx until all cultures neg • During admission, patient became agitated, tachypneic, O2 sat dropped; CXRLobar infiltrate; patient required intubation.
Case 6 (cont) • Take home points • In 1-3mo, WBC <5K or >15k/microL suggests need for LP • WBC <5K or >15k/microL, suggests need for admission with parental Abx until all cultures neg • Fever may be the only sign of occult PNA in young children.