Download
1 / 62
620 likes | 713 Vues
Babies Without a Test-Tube Dan C. Martin, M.D. University of Tennessee Health Science Center Memphis, Tennessee. Babies Without a Test-Tube www. DanMartinMD.com/bmhwbwtt.htm. Learning Objectives. Following the presentation “Babies With Test Tube” participants should be able to:

E N D
Babies Without a Test-TubeDan C. Martin, M.D.University of Tennessee Health Science CenterMemphis, Tennessee
Learning Objectives Following the presentation “Babies With Test Tube” participants should be able to: • Understand initial infertility evaluation. • Clarify evaluation and therapy with: • Normal History and Physical • Irregular Menses • Dysmenorrhea
Patients • Irregular Menses • Dysmenorrhea • Normal History and Physical
Patients • Irregular Menses PCOS • Dysmenorrhea Endometriosis • Normal History and Physical
Evaluation • Months • 6 Months • 12 Months • 36 Months • Available Resources • Age • 28 • 38 • 45
Disclosure • None
Off-Label Discussion • Clomiphene Citrate • Oral hypoglycemics • Estradiol • Progestins
One healthy baby Twins can be a major complication. Triplets are often a major complication. Goals
Evaluation • History • Physical • General Lab • Pregnancy Test, Pap Smear, GC and Chlamydia • CBC, TSH, prolactin, rubella, vitamin D* • Fertility Lab • Semen Analysis • Luteal Progesterone * Vitamin D deficiency is associated with pre-eclampsia and C-section for small pelvis
Evaluation • Day 3 FSH and E2 if age ≥38 (≥35) • HIV, RPR, fasting glucose, Type and Rh,free testosterone, testosterone, DHEAS, 17 OHP (follicular) • Sonogram • Sonohysterogram • Hysterosalpingogram (HSG) • Hysteroscopy • Diagnostic Laparoscopy
General • Prenatal Vitamins • Pregnancy test before any medication • Clomiphene Class X • Includes neural tube defects.Day 18 to 30 after ovulationUse folic acid up to 5 mg dailyStart 96 hours to 6 months before pregnant • Femara Class X
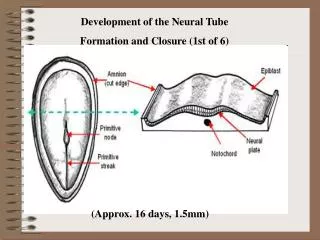
Windows of Opportunity Cervix (Tube) - Sex Endometrium -Implantation Ampulla - Fertilization
Windows of Opportunity • Cervical sperm survival – 2 to 8 days • Tubal sperm survival – 2 to 8 days? • Ampullary fertilization of egg – 6 to 7 hours • Implantation in endometrium – 6 to 7 days after LH surge
Windows of Opportunity • Cervix – 2 to 8 daysTubal Sperm also? • Ampullary Egg – 6 to 7 hours • Implantation – 6 to 7 days Estrogenized Tubal Environment Egg Release Estrogen proliferation and Progestin maturation of Endometrium Estrogenized Cervical Mucus
Basics • Sperm • An adequate number of spermatozoa must be deposited at or near the cervix at or near the time of ovulation, ascend into the fallopian tubes, and fertilize an ovum.
Basics • Ovary • A mature ovum must be released from the ovaries, ideally on a regular, predictable, cyclic basis.
Basics • Cervix • The cervix must capture, nurture, and release spermatozoa into the uterus that then travel into the fallopian tubes.
Basics • Peritoneum • The fallopian tubes must have a functional anatomic relationship with the adjacent ovaries to facilitate travel and capture.
Basics • Tubes • The fallopian tubes must be patent and also capable of timely transport of an embryo to the uterine cavity.
Basics • Uterus • The uterus must be receptive to embryo implantation and capable of supporting subsequent normal growth and development.
Ovulation • An LH (luteinizing hormone) surge begins 24 to 36 hours prior to ovulation and peaks 12 to 24 hours before ovulation. • Follicular rupture = It is the ovary’s job to make a cyst and rupture it. • Progesterone is increasingly produced after the LH surge • Secretory changes occur in the endometrium due to progesterone.
Ovulation • Pregnancy is absolute proof of ovulation. • Serum progesterones are 99%+ • 8 days after a positive ovulation test • 7 days after ovulation on a monitor • Day 21 and 24 if ovulation day is uncertain.
Patients • Irregular Menses • Dysmenorrhea • Normal History and Physical
Ovulation Disorders • PCOS • Hypothyroidism • Hyperprolactinemia • Weight Loss / Weight Gain
PCOS • Diagnosis is more clinical than lab. • Androgenism (hirsute, acne, central obesity) • Oligo-anovulatory • PCOM – polycystic morphology • > 12 follicles at 2 - 9 mm in at least 1 ovary • Volume > 10cc • Does not apply if on BCPs • If a follicle is >10mm, repeat scan next cycle • Elevated androgens • Androgens decrease with age • Decreased HDL and SHBG
PCOS • Treatment • Weight loss and exercise • Clomid (clomiphene citrate) (3 months) • Femara (aromatase inhibitor) (3 months) • Metformin (6 months) • Note that the combination of Metformin and Clomid are more productive at months 4-6 compared with months 1-3 . • Gonadotropins
PCOS • Weight loss • Poor results if BMI > 50 • Requires a dedicated program of diet and exercise • Use dieticians who work with diabetics • Liposuction of cutaneous fat is not the same as loss of visceral weight
Letrozole and ClomipheneBirth Defects • There is no increase in birth defects for letrozole or clomiphene if used when not pregnant. • Letrozole associated with fewer birth defects than clomiphene but this is not statistically significant. Tulandi T. Fertil Steril 85:1761, 2006
Clomiphene • Four ovarian responses to clomiphene • Ovulatory response • Anovulatory response • Ovulatory dysfunction • Luteinized unruptured follicle (LUF) • Ultrasound characteristics of ovulation
Ovulation Monitoring • Basal body temperature charting (BBTC) • Mid luteal phase serum progesterone • Urine LH hormone detection (ovulation kits) • Serial ultrasounds for follicular growth and collapse.
Sonographic Collapse • Collapse at 24 mm maximum or 21 mm mean with no stimulation –2 to 3 mm larger with clomiphene • Scan 1 to 2 days after collapse
Luteinized Unruptured Follicle • No Collapse • May respond to 10,000 to 20,000 IU HCG
Clomiphene Citratefor PCOS • Ovulatory rate - 80% • Pregnancy rate - 40% • Multiple rate • Twins - 5% • Triplets - < 1% • 80% of pregnancies occur in 4 cycles • 85% at 3 months if IUI
Patients • Irregular Menses • Dysmenorrhea • Normal History and Physical
Endometriosis Minimum Maximum Theoretical 1% 99% Family Practice 1% 15% Gyn Practice 30% 72%
Powder Burn? 1) Infiltrating dark and scarred or 2) Surface vesicles and hemosiderin. These lesions have different histology and behavior.
Theories • Retrograde Menstruation - Implantation • Mullerian Tissue Present at Birth • Coelomic Metaplasia • Vascular Metastasis • Lymphatic Metastasis
Theories Implantation Nisolle 1997 Nisolle 1997
Theories • Retrograde Menstruation • Pelvis • Bowel • Bladder • Appendix • Vagina • Sciatic Nerve • Diaphragm (Lungs)
Natural Progressioni f P r o g r e s s i n g • Implantation • Clear Blisters • Red Polypoid Blisters • Scarring and Blood Trapping • Collection of Old Blood • More Scar • Deep Infiltration
Histological Diagnosis Stroma Glandular Epithelium Old Blood Fibromuscular Scar