Download
1 / 14
140 likes | 276 Vues
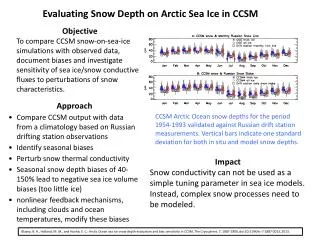
Objective. To determine whether nonresponsiveness to clopidogrel as revealed by high in vitro residual platelet reactivity after a 600 mg loading of the drug is predictive of drug-eluting stent thrombosis and cardiac mortality at long-term follow-up. Background.

E N D
Objective To determine whether nonresponsiveness to clopidogrel as revealed by high in vitro residual platelet reactivity after a 600 mg loading of the drug is predictive of drug-eluting stent thrombosis and cardiac mortality at long-term follow-up
Background The RECLOSE trial showed that nonresponsiveness to clopidogrel is predictive of drug-eluting stent (DES) thrombosis and cardiac mortality at 6 months. No data exist about the predictive value of long-term adverse events in patients with DES and clopidogrel loading non-responsiveness
Methods (1) • Consecutive pts receiving DES implantation and for whom platelet reactivity after clopidogrel loading was prospectively assessed. • All pts were compliant to 6-month dual antiplatelet treatment. • Blood samples for platelet reactivity assessment was obtained 12 to 18 hours from clopidogrel loading (600 mg). For patients receiving in the cath lab both the loading dose of clopidogrel and a IIb/IIIa inhibitor, blood samples were obtained after 6 days while patients were on 75 mg maintenance dose of clopidogrel.
Methods (2) Platelet-rich plasma was stimulated with 10 M ADP and aggregation was assessed using LTA. Patients with platelet aggregation by 10 µmol ADP ≥ 90th percentile of controls (70%) were defined as nonresponders.
Primary end-point: stentthrombosis (ARC definitions) • Definite Stent Thrombosis • Angiographicorpathologicconfirmation AND at least ONE additional criteria: • Acuteischemicsymptoms • Ischemic ECG changes • Elevatedcardiacbiomarkers • Probable Stent Thrombosis • Anyunexplaineddeathwithin 30 daysof stent implantation • Anymyocardialinfarctionin the territory of the implanted stent without angiographic confirmation of stent thrombosis • Possible Stent Thrombosis • Anyunexplaineddeathbeyond 30 days Secondary end-point: compositeofcardiacmortalityandstentthrombosis
Baseline Clinical Characteristics According to Responsiveness to Clopidogrel • OverallResp.Nonresp.p value • (n=804) (n=699) (n=105) • Age 69 ± 11 68 ± 11 71 ± 10 0.021 • Sex (male) 602 (75) 528 (76) 74 (70) 0.265 • Smokers 179 (22) 164 (24) 15 (14) 0.034 • Hypertension 501 (62) 434 (62) 67 (64) 0.748 • Diabetes mellitus 169 (21) 131 (19) 38 (36) <0.001 • Hypercolesterol. 405 (50) 347 (50) 58 (55) 0.291 • Prior MI 206 (26) 173 (25) 33 (31) 0.146 • Stable angina 275 (34) 242 (35) 33 (31) 0.520 • Unstable angina 312 (39) 258 (37) 54 (51) 0.004 • AMI 217 (27) 199 (28) 18 (17) 0.015 • Renal failure 87 (11) 73 (10) 14 (14) 0.374 • LVEF % 47±12 47±12 44±14 0.008
Baseline Procedural Characteristics According to Responsiveness to Clopidogrel • OverallResp.Nonresp. p value • n=804n=699n=105 • Multivessel disease 457 (57) 386 (55) 71 (68) 0.017 • Multivessel PCI 327 (41) 273 (39) 54 (51) 0.016 • Lesion treated 1369 1171 198 • Thrombotic lesion 177 (13) 166 (24) 11 (10) <.001 • Bifurcation lesion 371 (27) 318 (27) 53 (27) 0.909 • Chronic total occl. 106 (8) 86 (7) 20 (10) 0.180 • Lesion length > 20 mm 359 (26) 294 (25) 65 (33) 0.022 • Total stent length (mm) 38 ± 29 37 ± 29 44 ± 32 0.015 • Cypher stent 447 (56) 391 (56) 56 (53) 0.617 • Taxus stent 303 (38) 264 (38) 39 (37) 0.902 • Both stent types 54 (7) 44 (6) 10 (10) 0.218 • Glycoprotein IIb/IIIa 349 (43) 311 (44) 38 (36) 0.110
Cox Multivariate Analysis:Predictors of Stent Thrombosis at Six Months • HR(95%CI) P VALUE • Nonresponsiveness to clopidogrel3.08 (1.32-7.16) 0.009 • Acute myocardial infarction 2.41 (1.04-5.63) 0.041 • Total stent length (mm) 1.01 (1.00-1.02) 0.010 • LVEF per 1% increase 0.95 (0.92-0.98) 0.001
LONG-TERM SURVIVAL FOR PRIMARY END-POINT 100 97 ± 1 95 Log rank p <.001 89 ± 3 Event-free survival % (definite or probable stent thrombosis) 90 Responders Nonresponders 85 n=803 pts; median time follow-up 639 days - IQ 555-756 80 0 60 120 180 240 300 360 420 480 540 600 660 720 Time (days)
Incidenceofcardiacmortality nonresponders responders 11,4 % 3,8 % 2,7 % 1 % Cardiac mortality (after six months) Cardiac mortality (overall)
Incidenceofstentthrombosis nonresponders responders 11,4 % 2,6 % 2,8 % 0,3 % Stent thrombosis (after six months) Stent thrombosis (overall)
Conclusions High residual platelet reactivity after 600 mg loading dose of clopidogrel, as revealed by a single assessment with LTA, is a strong predictor of cardiac death and DES thrombosis.