Download

1 / 40
400 likes | 538 Vues
NHS Sickle Cell & Thalassaemia Screening Programme. Marie Coughlin Screening Lead March 29 th 2010. Today’s Session. Second of 6 Antenatal & Newborn sessions throughout 2010. Reasons for Today’s Session. As a result of ChaMPs commissioned review of screening

E N D
NHS Sickle Cell & Thalassaemia Screening Programme Marie Coughlin Screening Lead March 29th 2010
Today’s Session • Second of 6 Antenatal & Newborn sessions throughout 2010
Reasons for Today’s Session • As a result of ChaMPs commissioned review of screening • A need to further engage public health in Antenatal & Newborn Screening Programmes • At the request of public health screening leads • Part of C&M Screening Action Plan • Thought it useful to invite commissioners also
Aim of the Session • To increase knowledge base within public health and commissioning
Session Format • Overview of UK NSC/NWSHA structure • Overview of Sickle Cell & Thalassaemia Screening • Review of patient pathway • Data, performance and QA • Future developments • Questions/comments
Overarching Structure • UK NSC oversees 6 Antenatal & Newborn Screening Programmes • UK NSC has defined accountability & governance structure for SHA, PCT and provider • SHA coordinators with regional and national role • NWSHA coordinators now recruited; 1 x 8a, 1 x 8b – May/June start
Sickle Cell & Thalassaemia Screening • Programme was set up in England in 2001 following Government commitment in the NHS Plan (2000) • Is world’s first linked Antenatal and Newborn screening programme • Groundbreaking screening programme, not only reveals a condition but also identifys and systematically communicates carrier status • Screening available at 3 stages: • Men and women can ask for screening before they conceive • Parents offered screening during pregnancy • Babies screened shortly after birth (integrated with newborn bloodspot)
Programme Aims • To offer informed choice and to support people with decision-making in line with their beliefs and values • To offer timely screening to women (and couples) before 10 weeks of pregnancy • To identify 50% couples/women ‘at high risk’ by end of 12th week of pregnancy • To achieve the lowest possible childhood mortality and morbidity rates for sickle cell & thalassaemia disorders
Sickle Cell & Thalassaemia Explained • Sickle cell & thalassaemia are among England’s most commonly inherited genetic blood disorders. Sickle cell affects approx 12,500 people with an estimated 240,000 carriers • Around 700 people are affected by major thalassaemia with an estimated 214,000 carriers.
Sickle Cell & Thalassaemia Rebecca Till Screening Midwife Macclesfield District General Hospital 29th March 2010
Aim of Programme • Identify carrier status • Referral • Choices
Haemoglobinopathies • Inherited blood conditions • Affects haemoglobin
Inheritance Pattern Partner IS a carrier Partner who is NOT a carrier Not a carrier Not a carrier Carrier Carrier
Both Parents Carriers Carrier Carrier Affected Child Not a carrier
Carrier Status and Risk to Fetus Key: Serious Risk - Refer for counselling and offer prenatal diagnosis Less Serious Risk - Refer for counselling, further investigation maybe required No Risk - No further action Table based on work of B Modell
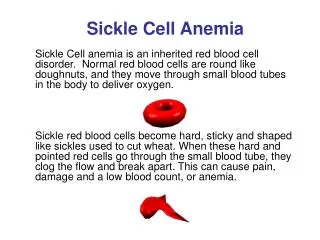
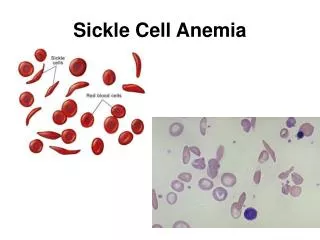
Sickle Cell • Affects haemoglobin • Oxygen carrying capacity • Normal Hb = HbA • Sickle Hb = HbS
Symptoms of Sickle Haemoglobin • Impairs oxygen passage through vessels • Hypoxia/crisis • Anaemia • Infections • Organ damage
Treatment • Pain relief • Prevent infections, organ damage and strokes • Hydorxeurea • Bone Marrow Transplant
Thalassaemia • Affects haemoglobin production • Life threatening • Life long treatment • Carrier • Thalassaemia major (severe)
Effects • Fatigue • Poor appetite • Slow growth • Jaundice • Enlarged spleen/liver/heart • Deformed/weak bones
Treatment • Blood transfusions • Chelation • Cure
Screening • Universal • High prevalence (> 1.5/10000) • Low prevalence (< 1.5/10000)
Pathway • Screen 8-10 weeks • Results • Action
Normal Result • Continue with pregnancy • Newborn bloodspot
Inconclusive Result • Inform woman • Assess risk • Consider partner testing
Carrier Result • Inform woman • Confirmation of carrier status • Offer partner screening
Affected • High risk pregnancy • Offer partner screening
Partner Screening Results Normal • Continue • Newborn bloodspot
Partner Carrier • Inform couple • Confirmation of carrier status • Confirmation of risk • Refer as ‘At Risk’ • Offer diagnostic testing
References • http://sct.screening.nhs.uk/ • http://sct.screening.nhs.uk/professional-resources • http://www.nice.org.uk/nicemedia/pdf/CG62FullGuidelineCorrectedJune2008July2009.pdf
Data & Performance • Trusts required to produce annual report – difficult to obtain copies • NSC produce annual report • 2008/2009 annual report in brief: • Due to crossed boundaries, robust patient pathways are crucial • Only 320 couples chose prenatal screening • Challenges engaging primary care in prenatal screening • Around 57% of fathers tested, unclear why number is low • Inadequate IT infrastructure • 350 babies born with sickle cell and over 9000 newborn carriers
Quality Assurance • QA in place for labs • Developing QA for the rest of the service • NWSHA coordinators will focus on QA
Future Developments • National office currently going through procurement process for training centres for labs • Status Codes Project underway to improve the link between parents and babies on current IT systems • NW policy being developed on how to improve the inclusion of transfused babies • IT failsafe system being piloted - receipt of sample by lab • Screening master class to include tips on commissioning high quality services – 1 July 2010 in London
Questions/Comments • With regard to QA, how do we assure our Boards that local programmes run satisfactorily?