Download
1 / 28
510 likes | 1.45k Vues
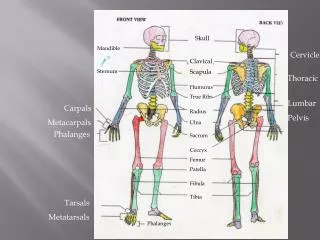
LATERAL SKULL BASE. AMOLENDA, Patricia G. Anatomy. Internal auditory canal with the facial nerve Jugular Foramen Foramen lacerum Foramen ovale Foramen spinosum. Clinical Examination. The symptoms of the diseases of the lateral skull base may cause deficits of CN 7, 8, 9, 10, 11

E N D
LATERAL SKULL BASE AMOLENDA, Patricia G.
Anatomy • Internal auditory canal with the facial nerve • Jugular Foramen • Foramen lacerum • Foramen ovale • Foramen spinosum
Clinical Examination • The symptoms of the diseases of the lateral skull base may cause deficits of CN 7, 8, 9, 10, 11 • CN testing • Oral cavity examination: CN 9 & 12 • Indirect laryngoscopy: CN 10, recurrent laryngeal nerve
Clinical Examination • Cochleovestibular Syndrome • Sensorineural HL • Tinnitus • Dysequilibrium and vertigo
Clinical Examination • Jugular Foramen Syndrome • CN 9: palatal deviation • CN 10: unilateral vocal cord paralysis and dysphagia • CN 12: tongue deviation toward the affected side, lingual atrophy, lingual fasciculations
Clinical Examination • Petrous Apex Syndrome • Triad • Purulent otorrhea • Stabbing ipsilateral facial pain (Trigeminal nerve irritation) • Diplopia (CN 6 palsy in petrous apex abscess)
Imaging Studies • CT Scan • Best for defining infiltration and destruction of bony structures • MRI • Better for defining and differentiating lesions especially tumor and inflammatory processes • Conventional Angiography • Assess disease processes in close proximity to major vessels • Embolization
Surgery of the Lateral Skull Base • Intracranial-intradural • Most common: suboccipital and retrosigmoid approach • Intracranial-extradural (Transtemporal) • Exposes the petrous pyramid through a temporal craniotomy • The dura is separated from the surface of the petrous pyramid and elevated away from it with the temporal lobe • Used in surgical treatment of temporal bone fractures or tumors of the internal auditory canal
Surgery of the Lateral Skull Base • Extracranial-extradural (Transmastoid and infratemporal)
Classification of Temporal Bone Fractures • Squama-mastoid Fractures • squLongitudinal temporal bone fracture • Transverse temporal bone fracture • Isolated meatal fracture
Squama-mastoid Fractures • Confined to the temporal squama and mastoid air cells • Auditory and tympanic cavity may also be involved
Isolated Meatal Fracture • Most often caused by a posterior displacement of the mandibular condyle • Usually due to a fall onto the chin • The fracture penetrates the posterior wall of the glenoid fossa and the anterior wall of the ear canal and is often associated with a condylar neck fracture
Longitudinal Temporal bone Fractures • Most common burst fracture • Caused by a diffuse, lateral traumatizing force (ex. Falls, brain trauma) • Fracture along the EAC and the anterior border of the petrous pyramid • Symptoms: otorrhea (blood or blood with CSF), hearing loss, bloody rhinorrhea, facial paralysis
Longitudinal Temporal Bone Fracture Diagnosis • Otoscopy: tearing of the meatal skin and TM, with bleeding into the ear canal • Clinical auditory testing (Weber test): lateralized to affected ear • Neurography: facial nerve function • Thin slice CT scan • Pure tone audiometry
Longitudinal Temporal Bone Fracture Complications • Meningitis, OM w/ TM perforation, facial nerve paralysis Treatment • Cover the ear with sterile dressing • Corticosteroids: facial paralysis • Surgical exploration
Transverse Temporal Bone Fractures • Fracture that runs across the petrous pyramid along the internal auditory canal and//or through the labyrinth • Caused by a traumatizing force in the frontal plane • Symptoms: severe vertigo, nausea and vomiting, deafness
Transverse Temporal Bone Fracture Diagnosis • Clinicalexamination: • Weber Test-Lateralized to the normal ear • spontaneous nystagmus towards normal side • Otoscopy: hemotympanum • CT Scan
Transverse Temporal Bone Fracture Complication • Meningitis, Facial nerve paralysis Treatment • Surgical closure
Otitis Media • most common inflammation and infection that affect the lateral skull base region • Cholesteatoma is one of its complications which arises from the middle ear and spreads to the lateral skull base
Tumors of the Temporal Bone • Paraganglioma • Primary Cholesteatoma or Epidermoid • Carcinoma of the Mucosa • Sarcoma • Lymphoma
Paraganglioma • Also glomustumor, chemodectoma • Most common tumor of the middle ear and adjacent lateral skull base • Arises from the paraganglia of the temporal region, most commonly in the area of the jugular bulb and along the neural plexus of the tympanic cavity • It may be located in the middle ear, jugular bulb, carotid bifurcation, and along the vagus nerve, and often extend to the temporal bone region
Paraganglioma • Manifestations: pulsatile tinnitus and conductive hearing loss, possible SNHL • Diagnosis: MRI, CT Scan, Angiography • Treatment: Surgery-subtotal petrosectomy
Tumors of the Internal Auditory Canal and Cerebellopontine Angle • Vestibular Schwanomma • Meningioma • Hemangioma • Lipoma
Vestibular Schwanomma • Slow-growing, benign, tumor arising from the Schwann cells of CN 8, affecting more commonly the vestibular nerve • Medial tumors arise from the intracranial part of CN8 while the lateral tumors are located in the internal auditory canal • Clinical hallmark is a unilateral hearing disorder which may consist of tinnitus, hearing loss and dysacusis
Vestibular Schwannoma • Medial schwannomas can occasionally produce trigeminal nerve symptoms such as facial pain or numbness in the jaw • Large tumors present with signs of brainstem compression and/or hydrocephalus with ataxia, nausea & vomiting • Diagnosis: • clinical examination: shows unilateral cochleovestibular d/o • Audiometry: shows retrocochlear impairment with lengthening of auditory brainstem reposnses • gadolinium enhanced MRI
Vestibular Schwanomma • <1cm: observe • 1-2.5cm: streotactic radiosurgery/ open surgery • >2.5cm: open surgery