Download
1 / 16
170 likes | 599 Vues
Blast and Crush Injuries Tintinalli Chap. 8. Blast and Crush Injuries. Stress Waves Created by the brief acceleration of a surface Transmitted deep into the body through the fluid of the tissues

E N D
Blast and Crush Injuries • Stress Waves • Created by the brief acceleration of a surface • Transmitted deep into the body through the fluid of the tissues • Damage occurs when the stress wave encounters tissues of different densities creating differential pressure forces, motion, stretching, and eventual tearing • Primary Blast Injury of the ears, lungs, and bowel • Shear Waves • Created by body deformation, which stretches tissues tangentially to the displaced surface • Blunt trauma and crush injuries
Blast Injuries • Ignition of explosives releases large amounts of energy in the form of expanding gases • These gases compress and superheat the surrounding air or water creating a shock wave • Solid Surfaces (Bone) • Shatter • Most body surfaces • “spring back” to original shape
Common Blast Injuries • Ear • TM bleeding/rupture • Fracture/dislocation of ossicles • Temporary or permanent hearing loss • Lungs • Hemo-/pneumothorax • Tension pneumothorax • Parenchymal hemorrhage • Pulmonary Contusion • Pneumatocele • Arterial Air Embolism (AAE) with subsequent distal ischemia • Bowel • Bleeding • Perforation and peritonitis
Common Blast Injuries • Other • Burns • Toxic inhalations • Traumatic amputations • Brain (TBI) • Not mentioned in Tintinalli • Leading nonfatal injury in the wars in Iraq and Afghanistan
Detection and Intervention • Airway Compromise • d/t depressed level of consciousness, facial/neck trauma, inhalation injury, or massive hemoptysis • Ventilatory Insufficiency • High-flow oxygen should be given to all victims with dyspnea, hemorrhage, or evidence of serious injury • CPAP • PPV • Can increase risk of AAE • External Hemorrhage • Control with direct pressure or tourniquets
Detection and Intervention • Tension Pneumothorax • Immediate needle thoracostomy • Tube thoracostomy if no improvement • Shock • Causes • Hemorrhage • Traumatic DVT and PE • Crush Syndrome • Sepsis (delayed care) • AAE causing brainstem stroke, MI, or spinal cord injury
Detection and Intervention • Arterial Air Embolism (AAE) • Consider if any of the following: • Localized ischemia of the skin/mucous membranes • Altered mental status • Focal neurologic deficits • Chest pain • Dysrrhythmia • Pulmonary edema • Abdominal pain • Hematuria • Sudden deterioration after an intervention (intubation)
Additional Evaluation • Pulmonary Primary Blast Injury • Dyspnea and chest pain • Pharyngeal petechiae or hemoptysis • Hemo-/pneumothorax • Pulmonary contusion • pneumatocele • Gastrointestinal Primary Blast Injury • Abdominal or testicular pain • N/V • Urge to defecate • Hematochezia
Management Caveats • External Hemorrhage is much more likely than airway compromise • MARCH • Air Embolism from positive-pressure ventilation is the most common cause of early death among immediate survivors • Positioning patient on the left side slightly forward prone may lower risk of AAE • Avoid rapid infusion of fluids because of high risk of pulmonary contusion
Disposition • Observe X 4 hours • If no chest or abdominal complaints and normal chest Xray and ABGs, may consider discharge with close follow-up • Admit all others
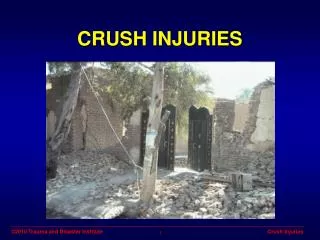
Crush Injuries • Acute Traumatic Ischemia (ATI) • More-appropriate term • Causes • Industrial Machinery Accidents • Building Collapse • Combat Injuries • Drug Overdose • Mining Accidents • Torture • Transportation and Construction Accidents
Pathophysiology • Disruption of adequate perfusion of the affected tissues • 2 Categories • Direct Macroscopic Muscular and Vascular Trauma • Microvascular Trauma • Hemorrhage, Edema, and Hypoperfusion • Leads to tissue hypoxia and ischemia • Cellular lysis results in the release of inflammatory mediators which further increase edema and hypoperfusion • Capillary blood flow is compromised at pressures exceeding 20 mmHg
Clinical Approach • Exam • Remove all clothing and jewelry • Palpate entire body for crepitus, swelling, or tenderness • Check capillary refill • Thorough neurologic examination • Re-assess frequently • Labs • CBC • BUN/Cr • Electrolytes • Phosphorus • Calcium • CK • Urinalysis • Urine myoglobin • Serial potassium, CK, and urine myoglobin
Management • Oxygen • Blood Transfusion • Continuous cardiac monitoring/pulse oximetry • NSS 250 cc bolus every 15 minutes until urine output is 2 cc/kg/hr • Furosemide 40-120 mg IV • Causes renal vasodilation, decreased oxygen demands by kidney, and increased renal flow
Disposition • Admit all patients • IV hydration • Serial labs • Close monitoring for compartment syndrome • Hyperbaric oxygen therapy, if available