Download
1 / 53
1.12k likes | 2.47k Vues
Impingement Syndrome. Mohammad Ali Tahririan Department of Orthopedics Kashani Hospital. History. History. Pain, weakness and loss of motion are the most common symptoms reported. Minor pain that is present both with activity and at rest

E N D
Impingement Syndrome Mohammad Ali Tahririan Department of Orthopedics Kashani Hospital
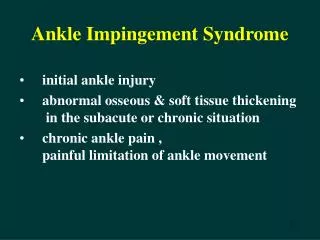
History Pain, weakness and loss of motion are the most common symptoms reported. Minor pain that is present both with activity and at rest Pain radiating from the front of the shoulder to the side of the arm Pain is exacerbated by overhead or above-the-shoulder activities. A frequent complaint is night pain, often disturbing sleep, particularly when the patient lies on the affected shoulder. The onset of symptoms may be acute, following an injury, or insidious, particularly in older patients, where no specific injury occurs.
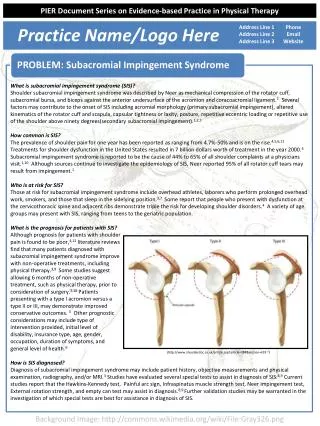
Primary impingement • Usually older than 40 years, • complain of anterior shoulder and upper lateral arm pain, with an inability to sleep on the affected side. • They have complaints of “shoulder weakness,” and difficulty performing overhead activities.
Primary impingement • On physical examination, patients may exhibit a loss of motion or weakness of rotator cuff strength secondary to pain. • They will usually have a positive Hawkins sign and a positive impingement sign as described by Neer. • The impingement test is performed by injecting 10 ml of 1% lidocaine into the subacromial space
Primary impingement • Intrinsic type • Extrinsic type • Tendinopathy(thickening of the RC) • Calcific tendinitis • Subacromial bursitis .Subacromial spur .Acromial fracture .Osacromiale .ACJ arthritis .Exostoses of the GT
Calcific tendinitis Calcific tendinitis is a painful, largely self-limited disorder of the rotator cuff in which the tendons are infiltrated with calcium deposits.
Calcific tendinitis Location This condition most frequently affects the rotator cuff of the shoulder. supraspinatus - 80% infraspinatus - 15% subscapularis - 5% periarticular soft tissues in addition to tendons ligaments capsule bursae
Calcific tendinitis Mostly asymptomatic Older than 30 y 10% of population 10% bilaterally F ˃ M
Calcific tendinitis Phase I—precalcification stage phase of formation Phase II—calcification stage resting phase Painful resorptive phase Phase III—postcalcificationphase
Calcific tendinitis Nonoperative treatment Nonoperative management is the initial treatment of choice. Nonoperative treatment usually includes physical therapy, exercises, anti inflammatory medications, and steroid injections. The efficacy of any of these treatment methods has not been proved, however. Corticosteroids have been suggested to abort the resorptive phase, returning the lesion to dormancy and setting into motion the factors necessary for recurrence.
Calcific tendinitis Operative treatment indications: symptom progression constant pain that interferes with activities of daily living absence of improvement after conservative therapy.
ultrasound-guided percutaneous needling +subacromial corticosteroid injection successful in approximately 70% of patients.
In a cadaver study of 140 shoulders, one third had full-thickness tears of the rotator cuff, 73% of which were in shoulders with type III acromions.
OsAcromiale • The acromion forms from 4 ossification centers that normally fuse by age 18 years, and acromion fuses to the spine at 20-25 y.
OsAcromiale • 1-15% of nl population • M˃F • B˃W • 30-60% Bilat. • Mean age: 50 y
The osacromiale may cause impingement because if it is unstable, it may be pulled inferiorly during abduction by the deltoid, which attaches here.
OsAcromiale • Optimal surgical treatment for symptomatic osacromiale is unclear.
The most common type treated mesoacromiale (94%)
The most common surgical technique: IF (60%) Excision (27%) Acromioplasty (13%) The most common concurrent surgical technique: RC Repair All techniques Improve clinical outcome
Treatment • NSAID,s • 1-2 subacromial cortisone injections • Physical therapy program focusing on stretching for full shoulder motion and strengthening the rotator cuff • Operative intervention may be indicated No response after 3-4 months
Treatment We use arthroscopic and occasionally open techniques. Principles: ■ Release (but not resection) of the coracoacromial ligament ■ Removal of the anterior lip and lateral edge of the acromion ■ Removal of part of the acromion anterior to the anterior border of the clavicle ■ Removal of the distal 1 to 1.5 cm of clavicle if significant degenerative changes are found
Secondary impingement • GH instability • Scapulothoracic instability Secondary impingement is a clinical phenomenon that results in a “relative narrowing” of the subacromial space.
Secondary impingement • Patients with secondary impingement are usually younger and often participate in overhead sporting activities such as baseball, swimming, volleyball, or tennis. • They complain of pain and weakness with overhead motions and may even describe a feeling of the arm going “dead.”
Secondary impingement physical examination • On physical examination, the examiner should look for possible associated pathology, including GH joint instability with a positive apprehension and relocation test or abnormal scapular function such as scapular winging or asymmetrical scapular motion.
Secondary impingement • Translation of the humeral head, typically anteriorly, resulting contact of the rotator cuff against the coracoacromial arch. GH instability
Secondary impingement • The loss of the stabilizing function of the rotator cuff muscles also leads to an abnormal superior translation of the humeral head (decreased depression of the humeral head during throwing and less “clearance”) and mechanical impingement of the rotator cuff on the coracoacromial arch .
Secondary impingement • In patients who have scapular instability, impingement results from improper positioning of the scapula with relation to the humerus. The instability leads to insufficient retraction of the scapula, which allows for earlier abutment of the coracoacromial arch on the underlying rotator cuff. Scapulothoracic instability
Secondary impingement • In patients with secondary impingement, treatment of the underlying problem should result in resolution of the “secondary impingement” symptoms. • A subacromial decompression here worsens the symptoms because the shoulder is rendered even more “unstable.”
Subcoracoid impingement • Gerber et al. suggested that this painful contact might be caused by a prominent coracoid, for which there may be numerous reasons, including idiopathic and iatrogenic conditions. • The iatrogenic form was most common in their series, and it was found in patients who had undergone a Trillat osteotomy of the coracoid for the treatment of anterior instability.
Physical findings Gerber Test -Tenderness over the coracoid -Positive coracoid impingement test. -Subcoracoid injection similar to the Neer impingement test
Internal impingement • In this condition, internal contact of the rotator cuff occurs with the posterosuperior aspect of the glenoid when the arm is abducted, extended, and externally rotated as in the position of the throwing motion.