Download
1 / 60
620 likes | 848 Vues
Clinical Indicator Goals Project. Shean Strong, QI Director Lisle Mukai, QI Coordinator ESRD Network 18 December 14, 2009. Clinical Indicator Goals Project . Background: Clinical Performance Measures (CPM) Project: Started in 1994 Random sampling of HD and PD patients

E N D
Clinical Indicator Goals Project Shean Strong, QI Director Lisle Mukai, QI Coordinator ESRD Network 18 December 14, 2009
Clinical Indicator Goals Project Background: Clinical Performance Measures (CPM) Project: • Started in 1994 • Random sampling of HD and PD patients • Collection of lab values • October – December (HD facilities) • October – March (PD facilities)
Clinical Indicator Goals Project • Laboratory values collected: • Hemoglobin • TSAT • Ferritin • URR • Kt/V • Albumin • Calcium • Phosphorus
Clinical Indicator Goals Project Uses of data: • Provides comparative data for facilities • National and local benchmarks • Allows the Network to identify areas for improvement within patient care • Allows the Network to assess the standard practice of the community for specific clinical indicators • The basis for setting Network goals
Clinical Indicator Goals Project Lab Data Collection (Elab) Project: • Started in 1998 • Nearly 100% sampling of HD and PD patients • Collection of lab values for the last quarter of each year • Same lab values collected as CPM project
Clinical Indicator Goals Project Uses of data: • Facility-specific generated reports • Provides comparative data for facilities • National and Network • Allow facilities to identify area(s) for improvement within patient care • Allows the Network to identify facilities who need to improve outcomes in specific clinical indicators
Clinical Indicator Goals Project Clinical Performance Goals-Network goals: • Goals are based on past performance, CMS thresholds and the NKF/KDOQI Clinical Practice Guidelines. • Provides a measurement tool to assess facility patient care processes and outcomes and identify opportunities for improvement.
Clinical Indicator Goals Project • Expectation is that facilities not meeting expected performance standards be monitored by the Network and develop internal quality monitors to promote continuous improvement.
Clinical Indicator Goals Project 2009-2010 Clinical Performance Goals:
Clinical Indicator Goals Project ** The goal was set by the MRB because PD patients lose albumin with the PD fluid.
Clinical Indicator Goals Project Quality Improvement Work Plan: (QIWP) • Requirement under the Network’s contract • Consists of 4 specific areas: • Vascular Access - Fistula First • Clinical Performance Measures • Network-specific quality improvement • Facility-specific quality improvement
Clinical Indicator Goals Project Clinical Indicator Goals Project: • Inclusion Criteria: • Facilities not meeting Network goals for anemia (4% of patients with Hgb < 10) • Patient census of > 50 patients (HD) • Patient census of > 20 patients (PD) • Exclusion Criteria: • Acute/transitional facilities • Patient census < 50 patients (HD) • Patient census < 20 patients (PD) • VHA facilities • Facilities participating in CROWNWeb Phase 2
Clinical Indicator Goals Project • Objective: • All facilities will be required to develop a QAPI (Quality Assessment and Performance Improvement) Plan utilizing the PDSA model to improve their sub-10 Hgb, implement those plans and monitor their progress. • Goal: Decrease the percentage of patients with a Hgb < 10 by at least 2 percentage points by April 2010. • Timeline: • October 2009 – April 2010
Clinical Indicator Goals Project • Due dates: • Run Charts (June–August 2009): due September 30, 2009: • QAPI: due January 15, 2010 • Quarterly Run Charts: • Oct-Dec 2009 (to be distributed in January) • Jan-Mar 2010 (to be distributed in April)
Clinical Indicator Goals Project Network Responsibilities: • Project Leader • Instruct/assist with the QI process • Distribute templates for RCA and PDSA • Distribute resources and evaluate their usefulness • Provide technical assistance as necessary • Conduct facility site visits as necessary
Clinical Indicator Goals Project Facility Responsibility: • Conduct a root-cause analysis and develop a QAPI Plan • Submit a copy of the QAPI plan to the Network • Implement QAPI plan and revise as necessary during the project • Monitor facility’s progress towards achieving the goal • Follow project timelines/due dates • Submit requested documents for the project in a timely manner
Quality Assessment and Performance Improvement Plan (QAPI) 494.110: (V626) Condition The dialysis facility must develop, implement, maintain and evaluate an effective, data driven, quality assessment and performance improvement program with participation by the professional members of the interdisciplinary team.
Quality Assessment and Performance Improvement Plan (QAPI) • Interdisciplinary Team: (minimum) • Physician • Registered nurse • Social Worker • Dietitian
Quality Assessment and Performance Improvement Plan (QAPI) (continued) Standard: Program Scope: 1. The program must include, but not limited to, an ongoing program that achieves measurable improvement in healthcare outcomes and reduction of medical errors by using indicators or performance measures associated with improved health outcomes and with the identification and reduction of medical errors.
Quality Assessment and Performance Improvement Plan (QAPI) (continued) Standard: Program Scope: 2. The dialysis facility must measure, analyze, and track quality indicators or other aspects of performance that the facility adopts or develops that reflect processes of care and facility operations.
Quality Assessment and Performance Improvement Plan (QAPI)(continued) Standard: Monitoring performance improvement: The dialysis facility must continuously monitor its performance, take actions that result in performance improvements, and track performance to ensure that improvements are sustained over time.
Quality Improvement Process The process involves: • Defining the problem • Investigating through gathering evidence • Identifying root causes • Implementing solutions • Monitoring those solutions to ensure they continue to prevent the original problem. Rootcauseanalybasics.com
Quality Improvement Process (continued) Root Cause Analysis (RCA): At its most basic, the process asks three questions, which together provide the framework of a root cause analysis investigation: 1. What was the problem? 2. What were the causes of the problem? 3. What actions should be taken to prevent the problem from occurring again? Rootcauseanalybasics.com
Quality Improvement Process (continued) • Root cause analysis can use a variety of techniques to uncover root causes, including cause mapping, change analysis, the Ishikawa fishbone diagram, 5 Whys, and others. • All are designed to analyze the elements affecting a particular outcome to determine the root causes. Rootcauseanalybasics.com
Quality Improvement Process (continued) Root Cause Analysis Investigations: • Every cause uncovered by RCA must be backed up by evidence. • RCA usually uncovers a system of root causes. • RCA uncovers specific causes and effects. • RCA results in executable, quantifiable solutions that may be monitored. Rootcauseanalybasics.com
Quality Improvement Process (continued) Root Cause Analysis Investigations: (continued) • RCA does not point blame at any one person or group, but simply identifies a system of causes and effects that lead to and incident. • RCA focuses on past events. Rootcauseanalybasics.com
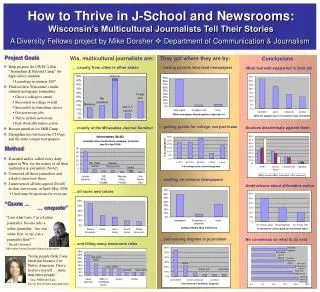
Quality Improvement Process(continued) Fishbone Diagram (aka: Cause and Effect Diagram) • The fishbone diagram will help to visually display the many potential causes for a specific problem or effect.
Quality Improvement Process (continued) Fishbone Diagram (continued) • The Cause-and-Effect diagram can be used by individuals or teams - most effective by a group. • The team assists by making suggestions of possible causes until no more causes can be suggested. • Once the entire fishbone is complete, a team discussion takes place to decide what are the most likely root causes of the problem.
Quality Improvement Process (continued) Fishbone Diagram: (continued) • Benefits of a fishbone diagram: • It helps teams understand that there are many causes that contribute to an effect. • It graphically displays the relationship of the causes to the effect and to each other. • It helps to identify areas for improvement. Institute for Healthcare Improvement
Quality Improvement Process (continued) 5 Whys: Repeatedly asking the question “Why” to peel away the layers of symptoms which can lead to the root cause of a problem. • Although this technique is called "5 Whys," you may find that you will need to ask the question fewer or more times than five before you find the issue related to a problem. Six Sigma (www.isixsigma.com)
Quality Improvement Process (continued) Benefits Of The 5 Whys • Help identify root cause of a problem. • Determine the relationship between different root causes of a problem. • One of the simplest tools; easy to complete without statistical analysis. Six Sigma (www.isixsigma.com)
Quality Improvement Process (continued) Whys And The Fishbone Diagram • The 5 Whys can be used individually or as a part of the fishbone diagram. • The fishbone diagram helps you explore all potential or real causes that result in a single defect or failure. • Once all inputs are established on the fishbone, you can use the 5 Whys technique to drill down to the root causes. Six Sigma (www.isixsigma.com)
Whys And The Fishbone Diagram Six Sigma (www.isixsigma.com)
Quality Improvement Process: (continued) Plan-Do-Study-Act: PDSA is the format the Network uses for developing a QAPI plan. ACT PLAN STUDY DO
Quality Improvement Process:(continued) • Quality improvement is a continuous cycle of planning, implementing strategies, evaluating the effectiveness of these strategies and reflection to see what further improvements can be made. Royal Children’s Hospital Melbourne – Clinical Quality & Safety
Quality Improvement Process:(continued) • PDSA approaches promote action by getting clinicians to reflect and brainstorm strategies that they hope will lead to improvement. • It also promotes evaluation of these changes once the strategies have been implemented. Royal Children’s Hospital Melbourne – Clinical Quality & Safety
Quality Improvement Process:(continued) • PDSA is a cycle of improvement that involves asking three key questions: 1. What are we trying to accomplish? 2. How will we know that a change is an improvement? 3. What changes can we make that will result in an improvement? NHS Scotland (www.clinicalgovernance.scot.nhs.uk
Quality Improvement Process:(continued) • Plan: • Set your objective for the project • Set goals to achieve (numerical goals and a target date) • Develop your plan on how you will improve your identified problem • Include a plan for collecting data • List data sources you will use to monitor your progress for the project
Quality Improvement Process:(continued) Plan (continued): • Write out the measure you will be using to analyze if you are achieving your goal. (numerical formula) Example: # of prevalent patients using AVF as primary access = AVF rate Total # of patients at the facility
Quality Improvement Process:(continued) Plan (continued): • Note the frequency in which you will conduct measurement of your progress • Note your baseline for comparison towards your goal
Quality Improvement Process:(continued) Do: • Implement your plan • Document problems and unexpected observations of your plan Study: • Analyze the results and compare it to the goal • This analysis should be conducted with the interdisciplinary team.
Quality Improvement Process:(continued) Act: • Is your plan successful? • How will you ensure continued improvement? • If it wasn’t successful, what needs to be changed based on what you have learned? • Should you continue to search for other root causes?
Plan-Do-Study-Act (PDSA) (continued) • The PDSA cycle is a continuous cycle. It allows you to frequently assess your plan and make revisions as necessary to achieve your goal. • Your plan should be reviewed at least monthly and/or when you realize that your strategy or activity is not working.
Quality Improvement Process:(continued) • Note your progress on your form so that you have a record of the strategies/activities you’ve attempted and results of those attempts as well as the revisions you have made to improve your plan.
Conditions for Coverage:Anemia Management The ESRD Conditions for Coverage include anemia as one of the clinical indicators required to be addressed in both the patient assessment and the facility’s QAPI program. FMQAI – Network 7