Download

1 / 0
30 likes | 412 Vues
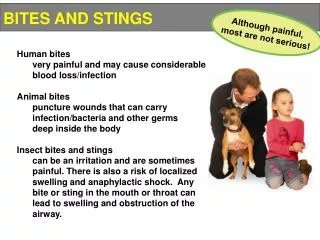
Animal Bites and Zoonosis. LTC Richard Ruck, MD Pediatric Infectious Diseases Walter Reed Army Institute of Research. Slides courtesy of: COL James F. Cummings MD Director , Global Emerging Infections Surveillance (GEIS). Disclosures.

E N D