Download
1 / 50
520 likes | 990 Vues
Contrast Induced Nephropathy and Nephrogenic Systemic Fibrosis. By Dr. HP Shum Apr 2008. Overview. Contrast induced nephropathy (CIN) Definition Pathogenesis Prevalence Risk factors Adverse outcome Prevention Nephrogenic systemic fibrosis. Definition of CIN.

E N D
Contrast Induced Nephropathy and Nephrogenic Systemic Fibrosis By Dr. HP Shum Apr 2008
Overview • Contrast induced nephropathy (CIN) • Definition • Pathogenesis • Prevalence • Risk factors • Adverse outcome • Prevention • Nephrogenic systemic fibrosis
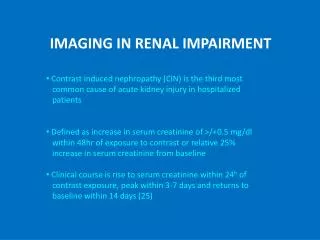
Definition of CIN • Including three components • Absolute or relative increase in serum Cr compared to baseline • Temporal relationship between the rise of Cr and exposure to contrast agents • Exclusion of alternative explanations for renal impairment >25% or 44umol/l increase of Cr level from baseline Within 48-72 hrs of exposure Cholesterol embolism, hypotension, UTI etc
Pathogenesis Use of adenosine antagonist Use of IVF / IOCM Use of IOCM Use of NAC Use of IVF / IOCM
4622 admitted to medical and surgical ward • 7.2% with baseline Cr >105umol/l AJKD, Vol 39, No 5 (May), 2002: pp 930-936
The overall incidence of CIN among general population is around 0.6-2.3% Radiology 1997; 203:605-610
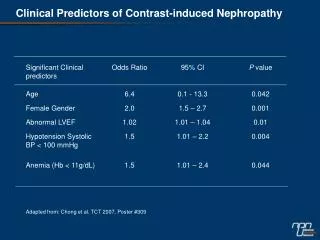
Pre-existing renal disease % of CIN JSurgRes 1992; 53:317-320
However… • Serum Cr varies with age, muscle mass and gender -> not reliable enough to identify patients at risk • Use Cockcroft or MDRD equation to calculate CrCl • eGFR <=60ml/min/1.73m2 is a reliable cut-off
DM + CRF Nephrol Dial Transplant 2007, 22, 819-826 NB: 400 pts, baseline GFR around 50ml/min
Volume of CM AmJCardiol 2004; 94:300-305 DM patients receiving PCI
Anemia Kidney Int 2005; 67:706-713
Type of CM Nephrotoxicity of iso-osmolar iodixanol compared with nonionic low-osmolar contrast media: meta-analysis of randomized controlled trials. (25 RCTs) Radiology. 2009 Jan;250(1):68-86 A meta-analysis of the renal safety of isosmolar iodixanol compared with low-osmolar contrast media. (26 RCTs) J Am Coll Cardiol. 2006 Aug 15;48(4):692-9 Iso-osmolar CM have lower CIN risk c/w low osmolar CM among patients with renal impairment or DM
CIN and mortality Mayo Clin Proc. 2008;83(10):1095-1100
IV Hydration • Decrease activity of the RAAS • Reduce vasocontrictive hormones like endothelin • Increase sodium diuresis • Decrease tubulo-glomerular feedback • Prevent tubular obstruction • Protect against reactive oxygen species • Dilute contrast medium in tubules
0.45% NaCl vs 0.9% NaCl N Tx regimen baseline Cr results P NS may be better than 0.45% NaCl
NaHCO3 vs NaCl • 12 RCTs, 1854 patients • Isotonic NaHCO3 decrease incidence of CIN (OR 0.39) c/w NaCl • No significant difference in needs for RRT and in-hospital mortality Am J Kidney Dis 2009 Apr; 53 (4), 617-627
Oral vs IVF Inconclusive, IVF may be better than oral route
NAC • Potent anti-oxidant • Scavenger of wide variety of oxygen derived free radicals • Prevent direct oxidative tissue damage
NAC beneficial for CIN prevention, especially those with renal impairment Ann Intern Med 2008; 148, 284-294
Adenosine antagonist (amiophylline and theophylline) • CM bind to renal adenosine receptor • Causing potent vasoconstriction • Impair renal blood flow • Adenosine antagonist may reverse renal vasoconstriction
Adenosine antagonist Benefit inconclusive, may be useful Ann Intern Med 2008; 148, 284-294
Dopamine and fenoldopam • Induce renal vasodilatation • Increase renal blood flow • Increase urine output
Dopamine and fenoldopam Not useful for CIN prevention Ann Intern Med 2008; 148, 284-294
Lasix Increase risk of CIN Ann Intern Med 2008; 148, 284-294
Renal replacement therapy • CM properties • Water solubility • Low protein binding • Low intracellular penetration • “middle size” molecules, much larger than urea and creatinine • 80% removal over 4hrs time by high flux dialyzer but much lower for low flux membranes • PD also remove CM but much slower (50% removal over 16 hrs)
Renal replacement therapy Int J Artif Organs 2008; 31, 515-524
RRT cannot prevent CIN Int J Artif Organs 2008; 31, 515-524
Conclusion • Prevent CIN by • Eliminate risk factors if possible • Use low or iso-osmolar CM • Use lower volume of CM • IV hydration (NaHCO3 > NS > 0.45 NaCl) • NAC
Nephrogenic Systemic Fibrosis • Scleroderma-like systemic fibrosing disorder • Originally termed “nephrogenic fibrosing dermopathy” due to its dominant skin findings but subsequently changed to NSF because of its systemic involvement • First case description in 1997
Peau d’orange skin changes Non-pitting edema with blister and bullae Contracture Cobblestoning and induration skin
Collagen bundles in thickened reticular dermis Extend through subcutaneous tissue Often involve fascia and skeletal muscle
NSF • No single causative agent or trigger was identified previously until 2006 • Five ESRF on HD developed NSF following exposure to Gadolinium-based contrast Nephrol Dial Transplant 21:1104-1108,2006 • Subsequently, numerous published studies and NSF registry have confirmed the link
Gadolinium • Silvery white rare earth metal • Strongly paramagnetic at room temp • Solution of organic gadolinium complex are used as MRI contrast
GBCM - pharmacokinetics • Molecular mass – 500-1000Da • Distributed in ECF only (0.26-0.28l/kg) • No protein binding • Excreted unchanged by kidney, renal clearance approx GFR in normal individual • Half life 1.3-1.6hrs but prolonged with low GFR
GBCM - clearance • Normal t1/2 1.3-1.6hr • CKD 3 (30-59) t1/2 5hr • CKD 4 (15-29) t1/2 9hr • CKD 5 (<15) t1/2 34hr • HD t1/2 2.1hr • PD without residual renal fx t1/2 53hr
NSF - Pathogenesis • Delay in GBCM excretion due to renal impairment • Spontaneous dissociation of the Gd-chelate complex into metal-ion and ligand • Free Gd forms precipitate with anions (PO4, CO3 etc) in the tissue • Internalized macrophages • Produce cytokines • Attract circulating fibrocytes • Induce tissue fibrosis
Procedure in which 10-15% of the patient's white blood cells are removed from the body by leukapheresis. White blood cells are exposed to a chemical agent that is activated by ultraviolet A (UVA) light. Activation by the UVA light induces an inhibition of the host response to foreign histocompatibility antigens. The photo-irradiated cells are washed free of the drug and re-infused into the patient. Indications: Cutaneous TCL, scleroderma


![ARMYDA-CIN Trial [ Atorvastatin for Reduction of Myocardial Damage during Angioplasty–Contrast-Induced Nephropathy ]](https://cdn0.slideserve.com/625136/slide1-dt.jpg)