Download
1 / 93
940 likes | 1.17k Vues
Sonographic Detection of Aneuploidy. Eric H. Dellinger, MD Director, Division of Maternal-Fetal Medicine Greenville Hospital System Greenville, South Carolina. Introduction. The Future of Science and Medicine: Exploring the extremes. Evolution of Ultrasound. Aneuploidy.

E N D
Sonographic Detection of Aneuploidy Eric H. Dellinger, MD Director, Division of Maternal-Fetal Medicine Greenville Hospital System Greenville, South Carolina
Introduction • The Future of Science and Medicine: Exploring the extremes
Benefits of Early Detection • Privacy issues • Decreased maternal bonding • Safer pregnancy termination • Higher detection rate
Nuchal Translucency • Clear space in posterior neck • Imaged between 11 and 14 weeks or when CRL is 36 to 84 mm • Nuchal thickening is associated with: • Aneuploidy • Anomalies • Infections • Metabolic and hematologic disorders
Incidence of chromosomal defects Nuchal translucency (mm) Total n Chromosomal defects (%) < 3.4 95,086 0.33 3.5 - 4.4 568 21.12 4.5 - 5.4 207 33.33 5.5 - 6.4 97 50.51 > 6.5 166 64.45 Snijders et al. 1998
Trisomy 21 Detection Rate • 96,127 patients studied • NT and age • Median age 31 years • 5% screen positive rate • 77% of affected fetuses detected Snijders et al, Lancet 1998; 352: 343.
Other Associations • Genetic syndromes: • Cornelia de Lange, Noonan, Smith-Lemli-Opitz, Apert • Anomalies: • Cardiac, diaphragmatic hernia • Adverse outcome: • Early demise • Targeted scan indicated if euploid
Cardiac defects Diaphragmatic hernia Omphalocele Duodenal atresia Esophageal atresia Skeletal dysplasias Lethal congenital arthryogryposis Smith-Lemli-Optiz syndrome Megacystis Fryn syndrome Joubert syndrome Meckel-Gruber syndrome VATER association Anomalies with Increased NT
NT and CHD • In 29,154 chromosomally normal fetuses, 56% of major abnormalities of the heart and great arteries were found in the subgroup with nuchal translucency above the 95th centile. • Nuchal translucency thickness at 11–14 weeks may constitute the most effective method of screening for cardiac defects. Hyett JA, et al, Br Med J 1999:318:81–5
NT and Cardiac Defects NT CHD per 1000 < 2.0 mm 1.9 2.0 to 2.4 mm 4.8 2.5 to 3.4 mm 6.0 > 3.4 mm 23 Bahado-Singh et al, Am J Obstet Gynecol. 2005 May;192(5):1357-61
Proper CRL is a MSLL MSLL = maximum straight line length
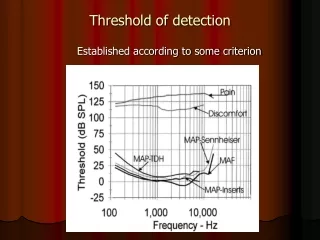
NT Interpretation From 10 - 14 weeks, the 99th percentile remains constant at 3.5 millimeters, independent of gestational age or crown-rump length. Nicolaides , Semin Perinatol. 2005;29(4):190.
NT thickness and chromosomal abnormalities other than trisomy 21
Adverse Outcome with Increased NT NT Poor Outcome 3.5 - 4.4 mm 32% 4.5 - 5.4 mm 49% 5.5 - 6.4 mm 67% > 6.5 mm 89% Ultrasound Obstet Gynecol 2001;18:9-17
Cutoff • 3 mm threshold identifies 80% of Downs • 5% SPR • High risk population • 95th percentile is a better threshold • NT between 95th and 99th percentile carries 3.7% risk of aneuploidy Br J ObGyn 1994; 101:782 Lancet 1998; 352: 343
Beware • NT cannot be obtained in all patients (~6%) • Fetal position • Maternal body habitus • Time constraints (allot 20 min) • Identify the amnion • Nuchal thickening may decrease over time
Essential for proper NT • Magnify the image until the fetal head and thorax occupy the whole screen. • Obtain a mid-sagittal view of the face. Minor deviations: non-visualization of the tip of the nose and visibility of the zygomatic process of the maxilla. • The fetus should be in a neutral position.
Essential for proper NT • Widest part of NT must be measured. • The crossbar of the calliper should be such that it is hardly visible as it merges with the white line of the border, not in the nuchal fluid. • Turn the gain down. This helps avoid placing the calliper on the fuzzy edge of the line which can underestimate the nuchal measurement.
Nasal Bone • Conflicting results in European vs. US studies • May reflect the technical difficulty of imaging • Review of over 35,000 nasal bone exams from 9 studies: • Successful study in 94.3% • Absent in 65% of Downs (0.8% of normals) Obstet Gynecol 2007; 110:300
Nasal Bone • The optimum time for nasal bone assessment is at crown rump length of 65 to 74 mm (13 to 13.5 weeks of gestation). • Absent nasal bone earlier in gestation could reflect delayed maturation, rather than actual absence of the structure. Ville, Am J Obstet Gynecol. 2006;195(1):1.
Doppler Umbilical Ductus
Tricuspid Regurgitation Normal Tricuspid Regurgitation
Anomalies and Aneuploidy Normal newborns 0.5% aneuploid Structural anomalies 11% aneuploid Am J Med Genet 1988;29:289
Type of Defect Matters Omphalocele with liver 3 of 34 aneuploid Omphalocele without liver 12 of 14 aneuploid AJR 1992;158:133; J Ultra Med 1989;8:299
Growth Restriction FindingAneuploid Isolated IUGR 2 % IUGR + anomaly 20 % Am J Obstet Gynecol 1993;168:547
Major Malformation • 33% of Down fetuses have one or more major malformations • Heart • CNS • GI • Face/neck • Hydrops Ped Clin N Am 1984;31:1331
Cardiovascular • 40-50% manifest heart anomalies