Download
1 / 1
10 likes | 132 Vues
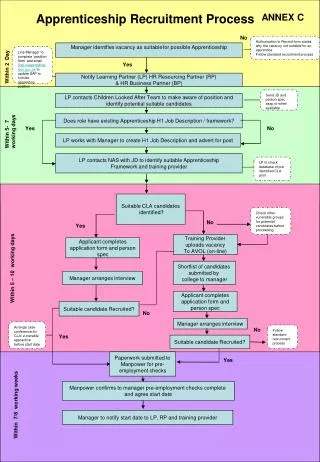
WPW no-no’s A denosine β -blockers C a 2+ Channel Blockers D igoxin Amiodarone – SAFE Procainamide if good VF Urgent/Delayed Cardiovert if >48hrs. ACLS Summary. † <48 hrs of A. Fib/A. Flutter Rate Control : Diltiazem OR Metoprolol (VF preserved)

E N D
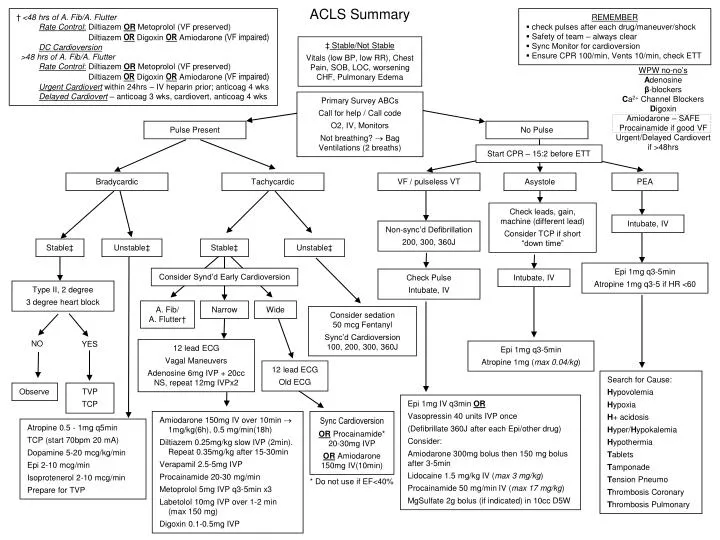
WPW no-no’s Adenosine β-blockers Ca2+ Channel Blockers Digoxin Amiodarone – SAFE Procainamide if good VF Urgent/Delayed Cardiovert if >48hrs ACLS Summary †<48 hrs of A. Fib/A. Flutter Rate Control: Diltiazem OR Metoprolol (VF preserved) Diltiazem OR Digoxin OR Amiodarone (VF impaired)DC Cardioversion >48 hrs of A. Fib/A. Flutter Rate Control: Diltiazem OR Metoprolol (VF preserved) Diltiazem OR Digoxin OR Amiodarone (VF impaired) Urgent Cardiovert within 24hrs – IV heparin prior; anticoag 4 wks Delayed Cardiovert – anticoag 3 wks, cardiovert, anticoag 4 wks REMEMBER • check pulses after each drug/maneuver/shock • Safety of team – always clear • Sync Monitor for cardioversion • Ensure CPR 100/min, Vents 10/min, check ETT ‡ Stable/Not Stable Vitals (low BP, low RR), Chest Pain, SOB, LOC, worsening CHF, Pulmonary Edema Primary Survey ABCs Call for help / Call code O2, IV, Monitors Not breathing? Bag Ventilations (2 breaths) Pulse Present No Pulse Start CPR – 15:2 before ETT Bradycardic Tachycardic VF / pulseless VT Asystole PEA Check leads, gain, machine (different lead) Consider TCP if short “down time” Intubate, IV Non-sync’d Defibrillation 200, 300, 360J Stable‡ Unstable‡ Stable‡ Unstable‡ Epi 1mg q3-5min Atropine 1mg q3-5 if HR <60 Consider Synd’d Early Cardioversion Check Pulse Intubate, IV Intubate, IV Type II, 2 degree 3 degree heart block A. Fib/ A. Flutter† Narrow Wide Consider sedation 50 mcg Fentanyl Sync’d Cardioversion 100, 200, 300, 360J NO YES 12 lead ECG Vagal Maneuvers Adenosine 6mg IVP + 20cc NS, repeat 12mg IVPx2 Epi 1mg q3-5min Atropine 1mg (max 0.04/kg) 12 lead ECG Old ECG Search for Cause: Hypovolemia Hypoxia H+ acidosis Hyper/Hypokalemia Hypothermia Tablets Tamponade Tension Pneumo Thrombosis Coronary Thrombosis Pulmonary Observe TVP TCP Epi 1mg IV q3min OR Vasopressin 40 units IVP once (Defibrillate 360J after each Epi/other drug) Consider: Amiodarone 300mg bolus then 150 mg bolus after 3-5min Lidocaine 1.5 mg/kg IV (max 3 mg/kg) Procainamide 50 mg/min IV (max 17 mg/kg) MgSulfate 2g bolus (if indicated) in 10cc D5W Amiodarone 150mg IV over 10min 1mg/kg(6h), 0.5 mg/min(18h) Diltiazem 0.25mg/kg slow IVP (2min). Repeat 0.35mg/kg after 15-30min Verapamil 2.5-5mg IVP Procainamide 20-30 mg/min Metoprolol 5mg IVP q3-5min x3 Labetolol 10mg IVP over 1-2 min (max 150 mg) Digoxin 0.1-0.5mg IVP Sync Cardioversion OR Procainamide* 20-30mg IVP OR Amiodarone 150mg IV(10min) Atropine 0.5 - 1mg q5min TCP (start 70bpm 20 mA) Dopamine 5-20 mcg/kg/min Epi 2-10 mcg/min Isoprotenerol 2-10 mcg/min Prepare for TVP * Do not use if EF<40%