Download
1 / 18
210 likes | 522 Vues
Trends in Morbidity for Lymphatic Filariasis in the Most Affected Area of Bangladesh. Midori Morioka 1 , Hossain Moazzem 2 , Kazuhiko Moji 3 , Yukiko Wagatsuma 1 1 University of Tsukuba, Department of Clinical Trial and Clinical Epidemiology,

E N D
Trends in Morbidity for Lymphatic Filariasis in the Most Affected Area of Bangladesh Midori Morioka1, Hossain Moazzem2, Kazuhiko Moji3, Yukiko Wagatsuma1 1University of Tsukuba, Department of Clinical Trial and Clinical Epidemiology, 2Institute of Allergy and Clinical Immunology of Bangladesh, 3Research Institute for Humanity and Nature 1-2 / September / 2012, 3th NTD Conference
Background Epidemiology: * Infection: 120 million people in 72 countries (WHO,2010) * Low human development index of 94% of those countries (Cristine Bonfim et al, 2009) * Second biggest factor related to impairment (WHO, 1995) Situation in Bangladesh: * Endemic area: 34 of 64 districts * Risk of infection: 70 million people * Infection: 20 million people (MOHFW Bangladesh, 2010) Figure1) Map of endemic areas in Bangladesh
Background Symptom of LF: 1. Asymptomatic microfilariaemia 2. Acute manifestation Acute episodic Adenolymphangitis (ADL) a) Acute filarial lymphangitis (AFL) b) Acute dermatolymphangioadenitis (ADLA) 3. Chronic manifestation Lymphedema, Elephantiasis, Hydrocele 4. Occult Filariasis etc
Background Acute manifestation:
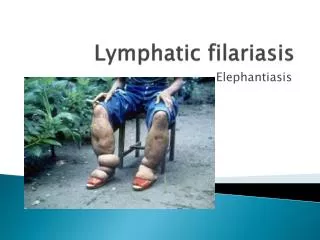
Background Chronic manifestation:
Background Eliminate LF by 2020 as started in the WHO initiative Elimination of LF by 2015 in Bangladesh Prevention Treatment To alleviate and prevent both the suffering and disability by morbidity control (MC) To interrupt transmission of infection by Mass Drug administration (MDA)
Methods Study area: Nilphamari Jaldhaka selected from6 upazilas Paurashava and Kanthali union selected from12 unites Figure2) Map of Jaldhakaupazila Paurashava:Ward2,3,6 Kanthali:Ward2,4 5 wards randomly selected
Methods Study sample: * Patients who had filarial acute or/and chronic manifestations * Patients aged less than 10 years - only registered, not interviewed chronic manifestation a) lymphedema with lower limb b) lymphedema with upper limb c) hydrocele d) lymphedema with breast e) lymphedema with sex organ f) other filarial symptoms
Methods Date collection: * Screened all households in 5 ward by 8 trained research assistants * Structure interview: socio-demographic information, medical and treatment history a) acute – ADL within previous and previous 12 months b) chronic – Dreyer staging system * Checked the validation by supervisor Data analysis: * Basic characteristics to show the distribution of lymphatic filariasis
Results Flow chart of sampling: 4,584 households728 residents listed 149 residents not directly observed 8 residents refused to join 31 residents aged less than 10 years 540 residents interviewedas patients 4 patients excluded because of misclassification 536 patients analyzed
Results Graph1. Disease Distribution n= 557 because 21 patients suffer from lymphatic filariasis with 2 parts. Child patients aged less than 10 years are not included.
Results Table1. Sex distribution 9 male patients suffer from lymphatic filariasis with 2 parts. 12 female patients suffer from lymphatic filariasis with 2 parts. Child patients aged less than 10 years are not included.
Results Graph2. Age distribution 21 patients suffer from lymphatic filariasis with 2 parts. Child patients aged less than 10 years are not included.
Results Table2. Disease distribution of child case aged 10-14 years length of illnessmean (±SD):5.2 (±3.4) years 31 child patients aged less than 10 years, that means to born after MDA, were also registered.
Results Graph3. Distribution of length of illness after MDA before MDA 21 patients suffer from lymphatic filariasis with 2 parts. The longest period is adopted for the patients affetced with both of right and left part. One is excluded because of only pain after hydrocele operation. Child patients aged less than 10 years are not included.
Results Graph4. Age of onset (clinical manifestation) - before and after MDA lymphedema with lower limb hydrocele 30.7 years (±12.7) 37.0years(±13.5) 29.7years(±16.5) Mean age(±SD) 24.6years(±13.7) Earlier age is adopted for the patients affected with both of right and left part. One is excluded because of only pain after hydrocele operation. 0-9 years: increased after MDA because of 31 child cases
Discussion and Conclusion * Disease magnitude (number of patients) hydrocele > lymphedema with limb sampling bias: working- aged male with hydrocele * Child case with hydrocele, family history * New case (chronic manifestation) despite of MDA, but not increasing * Age on onset getting higher after MDA, but increasing child case aged less than 10 years?? recall bias: before MDA * Further clinical assessment and statistical analysis especially focused on child hydrocele after MDA
Acknowledgement Dr. Moazzem and IACIB, Prof Moji, Prof Wagatsuma, Field research assistants and Patients Thank you for listening