Download
1 / 37
380 likes | 699 Vues
Crohn’s Disease. By: Jaspreet Deol, Laila Rkieh, Marice Zakhari, Sahar Noorzad. PHM142 Fall 2012 Coordinator: Dr. Jeffrey Henderson Instructor: Dr. David Hampson. CROHN’S DISEASE. Inflammatory Bowel Disease (IBD) Inflammation, swelling, and irritation of GI tract

E N D
Crohn’s Disease By: Jaspreet Deol, Laila Rkieh, Marice Zakhari, Sahar Noorzad PHM142 Fall 2012 Coordinator: Dr. Jeffrey Henderson Instructor: Dr. David Hampson
CROHN’S DISEASE • Inflammatory Bowel Disease (IBD) • Inflammation, swelling, and irritation of GI tract • Approximately 0.5% of the Canadian population have an IBD, highest reported prevalence rate • Jewish, highest risk; African Americans, lower risk • Prognosis: condition marked by periods of improvement followed by flare-ups • Diagnosed between ages 13-30 • Autoimmune disease • Decreased suppression of immune response for enteric bacteria and self-antigens
SYMPTOMATOLOGY • Pain/cramps • Caused by strictures (narrowing of the GI tract) • Narrowed passageway due to chronic inflammation and the formation of scar tissue • Bowel obstruction – nausea, vomiting • Diarrhea • Rectal bleeding • Anemia (Pernicious/Dietary) • Weight loss, reduced appetite • Fever, fatigue, skin lesions, join pain, delayed growth in children
COMPLICATIONS • Bowel obstruction • Complete/partial intestinal blockage caused by inflammation and accumulation of scar tissue • Ulcers • Chronic inflammation leading to holes/breaks in GI wall • Fistulas • Tunnels penetrating through the intestinal wall into surrounding tissue • External vs. Internal • Anal fissure • Malnutrition • Colon cancer • Arthritis, inflammation of eyes/skin, kidney stones, gall stones, inflammation of bile ducts
TYPES • Ileocolitis** • Ileitis • Gastroduodenal Crohn’s disease • Jejunoileitis • Crohn’s granulmatous colitis
DIAGNOSTIC TESTS PHYSICAL EXAMINATION INDICATORS: • Blood testWBC count: elevated with inflammation & infection Hematocrit and Hb levels: low in anemic state Vitamin B12, albumin, vitamin D: assess nutritional status • Stool test SPECIFIC TESTS TO DIAGNOSE CROHN’S • Colonoscopy: used to view the entire colon • Flexible sigmoidoscopy: lower colon and rectum • Computerized tomography (CT) scan: examines entire bowel and tissue outside the bowel -check for abscesses, fistulas
Factors Involved in Determining susceptibility to Crohn’s Disease
Genetic Susceptibility 1: Healthy Individuals • Intact Mucosal Barrier: In healthy individuals various protective measures are used to provide barrier to contact to invasive microorganisms: • These include secretions of mucous, intestinal trefoil factor (would healing, protection of epithelial barrier), as well as proteins IgA and defensins that prevent attachment/close association and proliferation of bacteria. • Tight Junctions are also present as a physical barrier to pathogen access.
Genetic Susceptibility 2: Healthy Individuals • Lack polymorphisms or defects in NOD2 gene. • Paneth cells in mucosal epithelia release NOD2 • Normal NOD2 is involved in activation of NFkB through homo-dimerization and binding to peptidoglycanmuramyldipeptide on bacteria. • Polymorphisms in NOD2 lead to a defect in the leucine rich repeat (LLR) that is involved in interacting with bacterial muramyldipeptide. • NFkB are involved in clearance of intracellular bacteria and production of alpha defensins. • Other loci have also been identified to play a role in Crohn's Disease: chromosome 12 (IBD2), chromosome 6 (IBD3), and chromosome 14 (IBD4).
Genetic Susceptibility 3: Healthy Individuals • Tolerance to self antigens or antigens on commensal/mutalistic bacteria.
Environmental Triggers and response • Includes contact to infectious agents such as bacteria, certain drugs/molecules, and even mutalistic bacteria normally present in gut. • Normal individuals are usually exposed to these, however mechanisms are present to deal with these factors effectively.
Cells To Know • Three Types of T-helper cells: TH1, TH2, TH3 -TH1 cells secrete Interfeuron-γ (IFN- γ), Tumour Necrosis Factor–α (TNF-α), Interleukins 1 and 6 (IL-1, IL-6) -TH2 cells secrete IL-4, IL-5, IL-10 -TH3 cells secrete Transforming Growth Factor – β (TGF-β) • Microfold cells (M cells): take up antigen from the small intestine and transport them to macrophages and dendritic cells on the basolateral side of the epithelial membrane • Antigen Presenting Cells(APCs): Dendritic cells and macrophages
In A Healthy Individual • Antigens within the intestine are uptaken by M cells and presented to APCs • Activation of TH2and TH3 cells overrides activation of TH1 cells • TH3 cells release TGF-β which results in B cells switching to the IgA isotype • This maintains oral tolerance
What Happens When Mucosal T-cells Are Activated In a Healthy Individual? 1. Cytotoxic T-cell Associated Antigen 4 (CTLA-4) signals regulatory T-cells to secrete IL-10 and TGF-β which mediate immunosuppressive activity No immune reaction to self-antigens, tolerance is achieved 2. Once a specific pathogen has been dealt with the activated T-cells undergo apoptosis • These pathways are defective in individuals with Crohn’s disease
In Crohn’s Disease • APCs exposed to bacteria release IL-12 in response to what would normally be an innocuous antigen • T cells interact with these APCs • TH1 cells differentiate and release cytokines such as IL-1, IL-6, TNF-α, IFN-γ • TNF-α binds TNF receptors on epithelial cells and macrophages • Activation of Inflammatory process
Events Associated by Cytokines Release from TH1 Cells • Effector cells are recruited (neutrophils, phagocytes) amplify the inflammatory response • IL-8 mediates migration of neutrophils through the epithelium and thus increase the permeability which results in increased uptake of bacteria from the lumen more tissue damage
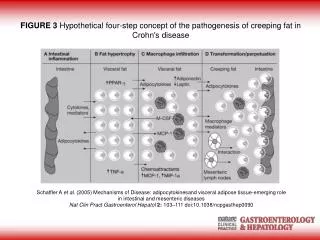
Role of IL-6 in Crohn’s Disease • IL-6 is released by TH1 Cells • IL-6 receptors or soluble IL-6 receptors released by macrophages interact with IL-6 • T cells become resistant to apoptosis • Leads to the accumulation of TH1 cells and cytokines released by them • Results in activation of matrix metalloproteinases (eg. stromolysin-1) which digest stromal tissue mediates tissue destruction, leads to fistulous tracts
Role of TNF-α in Crohn’s Disease • TNF-α is released by macrophages/monocytes and the differentiated TH1 cells. • Is a key player in Crohn’s disease and mediates its effects through expression of adhesion molecules (ex. Integrins), fibroblast proliferation, procoagulant factors, as well as the initiation of cytotoxic and acute-phase response. • Can also lead to release of IL-1β and IL-6 which are involved inTH1 cells pathway (associated with Crohn’s disease)
TREATMENT & MANAGEMENT • No cure • Involves treatment of active disease (flares) + maintenance of remission • Diet & nutrition • Non-Rx and Rx drug therapies • Surgery
DIET & NUTRITION • No specific diet proven to make symptoms better or worse • Recommendations • Eating small portions throughout day • Drinking plenty of water in small amounts • Avoiding fatty, greasy, fried foods and sauces • Limiting dairy products • Avoiding foods that cause gas (ex. beans) • Commonly prescribed supplements • iron • vitamin B12
DRUG THERAPY • Non Rx treatment of acute symptoms • Diarrhea, gas • Acetaminophen for mild pain (not NSAIDS!) • Supplements • Rx treatment of flares and for remission • Antibiotics • Aminosalicylates • Corticosteroids • Mercaptopurine • Monoclonal Antibodies
AMINOSALICYLATES • Mild to moderate CD • Active form: 5-ASA - anti-inflammatory • First line therapy due to lower side effects • Ex. Mesalazine, Sulfalazine
CORTICOSTEROIDS • Moderate to severe CD • Anti-inflammatory • Suppress inflammatory genes that are activated in chronic inflammatory diseases by reversing histone acetylation, among other mechanisms • Used sparingly due to side effects • Reduce ability to fight infection* • Ex. Prednisone, Budesonide
MERCAPTOPURINE • Remission: duration of action is months • Purine analogs • Exact mechanism unknown • Interference with nucleic acid metabolism in immunological sequence that follows antigenic stimulation • Ex. Azathioprine, 6-MP
TNF-α INHIBITORS • Severe CD – unresponsive to other treatments • Biologic therapies: Monoclonal Antibodies • Anti-TNF-α antibodies bind to TNF-α to prevent binding and activation of TNF receptors (neutralisation) • Inactivation down regulates inflammatory reactions of autoimmune diseases • May cause apoptosis of TNF-α expressing activated T cells • Treatment of fistulising disease (closing & maintenance of closure) & inflammation
ANTI-TNF-α MONOCLONAL ANTIBODIES Infliximab (Remicade) Adalimumab (HUMIRA) Fully human antibody Subcutaneous injection ONLY (self) • Mouse-human chimeric antibody • IV ONLY (clinic/hospital)
SURGERY • Reserved for complications or when disease that resists treatment is confined to one removable location (bowel resection) • Complications requiring surgery may include • Hemorrhage • Fistulas • Abscesses • Strictures • Colon cancer
Summary • Crohn’s Disease is characterized by inflammation, swelling, and irritation of the GI tract. • Common symptoms include pain/cramping, vomiting, diarrhea, rectal bleeding, and anemia. Strictures, responsible for pain and cramping, are narrowed passageways within the GI tract, caused by chronic inflammation and the accumulation of scar tissue.Healthy individuals have an intact mucosal barrier, whereas those with Crohn’s disease have a permeable barrier. • Polymorphisms in NOD2 gene are involved in Crohn’s Disease • In Healthy individuals activation of TH2 and TH3 cells overrides activation of TH1 cells that are involved in Crohn’s disease. • TH1 cells differentiate and release cytokines such as IL-1, IL-6, TNF-α, IFN-γ • IL-6 is involved with T cell resistance to apoptosis. • Matrix metalloproteinases leads to the fistulous tracts seen in Crohn’s disease patients due to tissue destruction. • • No cure; management involves treatment of active disease and maintenance of remission • • Antibiotics, anti-inflammatory and immunosuppressant drugs can be included in treatment • • Monoclonal antibodies are administered for neutralization of TNF-a to combat inflammation and fistulising disease; Infliximab (Remicade)-->mouse-human chimeric, Adalimumab (HUMIRA)-->human
References • Balfour, S.R. (2007). Bacteria in Crohn’s disease: mechanisms of inflammation and therapeutic implications. Journal of Clinical Gastroenterology, 41, S37-S43. • Bernsetin C., Blanchard, J., Fedorak, R., Israel, D., Jackson, M., Koehoorn, M., MacKenzie, A., Svenson, L., & Wajda, A. (2006). The epidemiology of inflammatory bowel disease in Canada: a population-based study. American Journal of Gastroenterology, 101 (7), 1559-1568. • Crohn’s Disease. (2012). In A.D.A.M. Medical Encyclopedia online. Retrieved from http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001295/ • Crohn’s and Colitis Foundation of America. (2012). Types of Crohn’s Disease and Associated Symptoms. Retrieved from http://www.ccfa.org/what-are-crohns-and-colitis/what-is-crohns-disease/types-of-crohns-disease.html • Goa, B., Saba, T.M., Tsan, M.F. (2002). Role of αvβ3-integrin in TNF-α-induced endothelial cell migration. American Journal of Physiology, 283,C1196-C1205. • Henderson, J. Hypomethylation, Folic Acid Metabolism, and Vitamin B12 [PDF Document]. Retrieved from Lecture Notes Online Website: http://phm.utoronto.ca/~jeffh/phmunit4cb.pdf • Kanai, M., Mullen, C., Podolsky, D.K. (1997). Intestinal trefoil factor induces inactivation of extracellular signal-regulated protein kinase in intestinal epithelial cells. American Journal of Physiology, 95, 178-182. • Mayo Foundation for Medical Education and Research. (2011). Crohn’s Disease. Retrieved from http://www.mayoclinic.com/health/crohns-disease/ • Műzes, G., Molnár, B., Tulassay, Z., and Sipos, F. (2012). Changes of the cytokine profile in inflammatory bowel diseases. World Journal of Gastroenterology, 18(41), 5848-5861. • National Digestive Diseases Information Clearinghouse. (2011). Crohn’s Disease (NIH Publication No. 12-3410). Betheseda, MD: U.S. • Sengupta, N., MacDonald, T.T. (2007). The role of matrix metalloproteinases in stromal/epithelial interactions in the gut. Physiology, 22(6), 401-409. • Shanahan, F. (2002). Crohn’s Disease. The Lancet, 359, 62-69. Retrieved from: http://journals1.scholarsportal.info.myaccess.library.utoronto.ca/tmp/12075267405419499946.pdf • "National Digestive Diseases Information Clearinghouse (NDDIC)." Crohn's Disease. National Institutes of Health, 18 Jan. 2011. Web. 17 Nov. 2012. <http://digestive.niddk.nih.gov/ddiseases/pubs/crohns/>.