Download
1 / 73
730 likes | 733 Vues
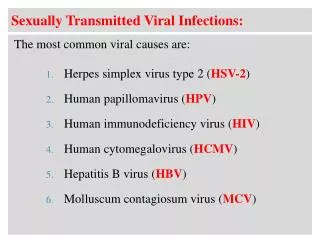
Unit 4 Part 5 Viral Infections. Terry Kotrla, MS, MT(ASCP)BB. Herpes Virus Group. Include 8 viruses that cause disease. May result in sub-clinical infections Capable of establishing latent infection. May be reactivated under appropriate conditions. Herpes Virus Group.

E N D
Unit 4Part 5 Viral Infections Terry Kotrla, MS, MT(ASCP)BB
Herpes Virus Group • Include 8 viruses that cause disease. • May result in sub-clinical infections • Capable of establishing latent infection. • May be reactivated under appropriate conditions.
Herpes Virus Group • We will discuss the following: • Epstein-Barr virus • Cytomegalovirus • Herpes simplex virus type I and II • Varicella-zoster virus
Epstein-Barr Virus (EBV) • Spread through oral transmission • Cause of Infectious Mononucleosis. • Other Diseases include: • African or Burkitt’s lymphoma • Nasopharyngeal carcinoma • B cell lymphoma
Infectious Mononucleosis • Acute self-limiting infection of the RE system • Four to 7 week incubation • Enlarged lymph nodes in the neck. • Sore throat, fever, rash • Malaise and extreme tiredness • Liver and spleen involvement and enlargement.
Infectious Mononucleosis - Lab • Hematology: • High WBC, • Over 20% atypical reactive lymphocytes also known as Downey cells. • Positive mono (heterophile antibody) test. • Negative mono test do tests for antibodies to EBV associated antigens.
Infectious Mononucleosis • Downey cells may be present
Heterophile Antigens/Antibodies • Heterophile antigens are a group of similar antigens found in unrelated animals, i.e., man, sheep, horse, dog cat, mouse. • Heterophile antibodies produced against heterophile antigens of one species will cross react with others.
Heterophile Antigens/Antibodies • Forssman antigen is an example of a heterophile antigen and is found on the RBCs of many species (guinea pig, dog, cat, mouse, sheep, fowl, horse) • Forssman antibodies formed against Forssman antigens will agglutinate sheep RBCs.
Paul Bunnell Test • Simple titration of sheep cell agglutinins. • Serial dilutions of patient serum. • Add sheep RBCs. • Positive indicates presence of heterophile antibodies. • Not specific for IM, screening test only.
Davidsohn Differential • Used to determine heterophile antibody present. • Add patient serum to one tube with guinea pig kidney and another with beef red blood cells. • Beef RBCs have IM antigen. • Guinea pg kidney have Forssman antigen. • Harvest serum and test with sheep cells.
Davidsohn Differential* To be considered absorbed there must be greater than a three tube difference between the presumptive titer and the differential titer.
Advantages When properly performed, this test is specific for Infectious Mononucleosis False-positive results are rare. Disadvantages Davidsohn Differential test is very time consuming and burdensome. Davidsohn Differential
Infectious Mono Slide Tests • It was discovered that horse RBCs possess antigens which react with the antibody associated with IM. • Patient serum mixed with horse RBCs, agglutination is positive. • Latex agglutination, coat particles with EBV antigens. • Not diagnostic, must look at total clinical picture.
EBV Antigens • Early antigen (EA) • Capsid antigen (VCA) • Membrane antigen (MA) • Nuclear antigen (EBNA)
EBV Specific Antibodies • EBV specific antibodies may be measured. • Pattern of appearance of EBV antigens. • Most valuable is IgM antibody to viral capsid antigen (VCA), indicates a current infection (best marker), lasts about 12 weeks. • Can also detect anti-early antigen (EA) (recent infection) and anti EB nuclear antigen (EBNA) (older infection). • ELISA and IFA most commonly used
African or Burkitt’s Lymphoma • EBV has been strongly implicated • Malignant B-cell neoplasm • presents as rapidly growing tumor of the jaw, face or eye • grows very quickly, and without treatment most children die within a few months • Rare in US, equatorial Africa. • Also associated with HIV infection.
African or Burkitt’s Lymphoma • Although BL is a very rapidly growing tumour it responds well to treatment. • Three pictures: before treatment, 3 days and 6 days after treatment
Nasopharyngeal Carcinoma • Endemic in South China, Africa, Arctic Eskimos • This is a malignant tumour of the squamous epithelium of the nasopharynx. • 100% contain EBV DNA • Rates are less than 1 per 100,000 in most populations • Nasopharyngeal carcinomas are found in association with reactivation of latent Epstein-Barr Virus. • The exact mechanisms of association are unknown
B-Cell Lymphoma • In most individuals infected with EBV, the virus is present in the B-cells, which are normally controlled by T-lymphocytes • When T-cell deficiency exists, one clone of EBV-infected B-lymphocytes escapes immune surveillance to become autonomously proliferating. • EBV induced B cell lymphomas are most prevalent in immunocompromised patients.
Oral Hairy Cell Leukoplakia • HIV infection stimulates reactivation of pre-existing, latent EBV infection. • Causes viral infection of the oral cavity. • Indicator of HIV infection as well as of a person's lessening or weakening immunity
Cytomegalovirus • Human Herpesvirus 5 (HHV-5) • Transmission occurs from person to person. • Close intimate contact • Sexual contact • Perinatally • Breast milk • Organ transplant • Blood transfusion
CMV Clinical course • Symptoms resemble IM • In babies may cause life threatening illness • Patients with deficient immune systems • AIDS patients • Transplant patients
Cytomegalovirus • Perinatal transmission occurs in 10%. • If infected may cause multitude of symptoms • Petechiae • Jaundice • Hepatosplenomegaly • Neurological abnormalities • Moratlity rate 5 percent • Survivors may exhibit hearing loss, visual impairment and mental retardation.
CMV Immunologic response • Test for CMV antibody using paired serum samples • IgM antibodies produced against early and intermediate-early (IE) CMV antigens, last for 3 to 4 months. • IgG appear shortly after and peak at 2 to 3 months.
CMV Laboratory Diagnosis • Range from culture and cytologic techniques to DNA probes, PCR and serologic techniques. • Detection of antibodies indicator of recent or active infection. • Viral cultures
CMV Lab Diagnosis • Detection of CMV antigen in cells using IFA • ELISA to detect antibody to CMV • Other • fluorescence assays, • indirect hemagglutination, and • latex agglutination • False positives can occur due to RA and Epstein-Barr antibodies
Herpes Simplex Virus (HSV) • Most exposed in childhood • Possesses viral latency – hibernation • Two types: HSV-1 and HSV-2
HSV-1 • Transmitted from person to person by saliva or direct contact. • Cold sores around the mouth most common. • Reactivation - may have several episodes of cold sores during a lifetime
HSV-1 • Symptoms • tingling • Numbness • Itching • Blister forms, breaks, crusts over • Reactivation usually caused by stress. • Conjunctivitis, keratitis and herpetic whitlow may occur.
HSV-2 • Results in Herpes genitalis - lesions BELOW the waist. • Transmitted intimate sexual contact or perinatally. • Symptoms • Pain • Tenderness • Itch • Fever • Headache • Lymphadenopathy • Malaise
HSV-2 • Blisters appear • Males – penis • Females – vagina and cervix • Both – thighs buttocks • Painful, lasts 1-3 weeks • Virus lies dormant in nearby nerves and reactivated.
HSV – 2 • Can be fatal in infants • Woman with active infection needs C-section. • Infants with localized infections have 70% mortality rate • Disseminated neonatal herpes most lethal form.
Laboratory Testing for HSV • Recovery of virus from culture • Direct examination of cells from lesion using IF or immunoperoxidase stain • DNA probes • ELISA • Latex agglutination • RIA • Indirect IF • Serology NOT very useful
Varicella-Zoster Virus • Two different manifestations of the same virus. • Varicella is the primary infection, causes chicken pox • Herpes Zoster causes shingles and is due to reactivation of the latent virus
Varicella • Fever and vesicular exanthema • Small, itchy blisters surrounded by inflamed skin. • Begins as one or two lesions and spreads. • Number of lesions vary greatly. • Blister dries out and forms a scab.
Chicken Pox • Secondary complications due to infection most common. • May also result in pneumonia, encephalitis and hepatitis. • Very serious for immunocompromised children • Vaccine now available
Shingles • Chicken pox – virus goes latent • Reactivated later in life • Weakened immune system • Aging • Other factors
Shingles • The typical rash of shingles begins as redness(erythema) followed by the appearance of blisters. • Eruptions follow the path of an infected nerve. • The trunk is the area affected in 50% to 60% of cases. • Skin may be extremely sensitive to touch
VZV Laboratory Testing • Important to distinguish VZV from other infections • PCR • Direct Fluorescent Antibody staining • Viral culture • IgG and IgM antibody test by ELISA
Rubella Virus • RNA virus with 3 major structural proteins, E1, E2, and C. • Incubation 2- 3 weeks • Highly contagious, spread through respiratory tract. • Causes German measles • Rubella vaccine has resulted in 99% decline in infections.
Rubella Symptoms • Mild and difficult to notice • Mild fever • Headache • Stuffy or runny nose • Red eyes • Enlarged and tender lymph nodes • Pink rash begins on face, spreads to trunk then arms and legs, disappears in same order. • Aching joints