Download
1 / 45
550 likes | 1.43k Vues
Tools of Prenatal Diagnosis. Julie Moldenhauer, MD Reproductive Genetics Maternal Fetal Medicine Obstetrics and Gynecology. Objectives: Discuss various prenatal screening and testing tools Discuss the timing of the various tools in gestation Discuss benefits and risks of various options

E N D
Tools of Prenatal Diagnosis Julie Moldenhauer, MD Reproductive Genetics Maternal Fetal Medicine Obstetrics and Gynecology
Objectives: • Discuss various prenatal screening and testing tools • Discuss the timing of the various tools in gestation • Discuss benefits and risks of various options • Review the difference between screening and testing
Baseline Risk for Birth Defects in the General Population is 3-5%
Structural Abnormalities • Congenital heart disease • Spina bifida • Gastroschisis • Chromosomal Abnormalities • Trisomy 21 • Triploidy • Infections • Parvovirus • Cytomegalovirus • Toxoplasmosis • Growth Abnormalities • Hematologic Abnormalities • Anemia • Thrombocytopenia • Functional Defects • Arthrogryposis • Renal dysfunction • Syndromes • Skeletal Dysplasia • Diabetic embryopathy What Can We Diagnose in the Prenatal Setting?
Prenatal Diagnosis Tools • History**** • Personal History • Family History • Population Screening • Serum Screening • Ultrasound • Fetal MRI • Invasive Diagnosis • Chorionic villus sampling • Amniocentesis Oaklandcc.edu
History is a Screening Tool! • Medication Exposures • What medications? • When was the exposure? • Environmental Exposures • Does she work in a preschool and was exposed to parvovirus? • Is she exposed to high doses of radiation? • Family History • Brother with hemophilia • Uncle with cystic fibrosis • Ethnic background • Consanguinity • Maternal Age • > 35 years at delivery • Obstetric History • Prior baby born with Down syndrome • Prior stillbirth • Medical History • Is mom diabetic? How well controlled is her sugar? • Does she have PKU? • Is she hypertensive?
As maternal age increases, the risk for aneuploidy increases. This is due to maternal meiotic nondisjunction. Maternal age > 35 at the time of delivery is considered “Advanced Maternal Age” or AMA
Down syndrome phenotype caused by trisomy 21 Down syndrome phenotype caused by 14;21 translocation • The risk for recurrence of chromosome abnormalities is dependent upon the genetic mechanism involved. • Trisomy: 1% or maternal age-related risk • Translocation: • Maternal carrier: 10-15% • Paternal carrier: 2%
Maternal Diabetes: Reproductive Risks • Obstetric • Spontaneous preterm labor • Polyhydramnios • Preeclampsia (15-20%) • Intrauterine growth restriction • Shoulder dystocia • Cesarean delivery • Fetal and Neonatal • Congenital anomalies: 6-12% • Intrauterine fetal demise • Macrosomia – Shoulder dystocia • Growth restriction • Hyperbilirubinemia • Hypoglycemia • RDS • Polycythemia • Organomegaly • Long term – obesity and carbohydrate intolerance Caudal Regression Syndrome ACOG Practice Bulletin #60: Pregestational Diabetes Mellitus, March 2005
Teratogen Exposure • Examples: • Accutane • ACE inhibitors • Lithium • Antiepileptic drugs (AEDs) • Anticoagulants: warfarin • Antidepressants • Methotrexate • Thalidomide • Fetal effects are timing and dose dependent • Each medication is assigned a pregnancy category based on available data; A-D, X • www.Reprotox.org • www.otispregnancy.org
Ultrasound images of fetal hydrops – abnormal collection of fluid in multiple body compartments. Mom works at a daycare where there was a Parvovirus B19 or Fifth Disease outbreak 4 weeks ago. Parvovirus causes fetal aplastic anemia that can be life-threatening.Suspicion of diagnosis by altered maternal serum titers of Parvo IgG and IgM and confirmed by amniotic fluid PCR for Parvo. Confirmed Parvo infection in a fetus with hydrops can be treated with intrauterine blood transfusions.
= MR = asthma = TSC 6 2 2 n n
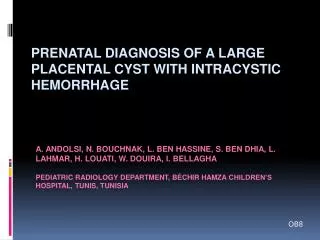
Fetal Ultrasound Showing Cardiac Rhabdomyoma Fetal MRI Showing Tubers Prenatal Findings Consistent with Tuberous Sclerosis Confirmed as Neonate
Screening for Genetic Disease Ethnic Group Disease African American Sickle Cell Disease: 1/12 Mediterranean Beta-Thalassemia: 1/30 Southeast Asian Alpha-Thalassemia: 1/20 Caucasian Cystic Fibrosis: 1/25
ASHKENAZI JEWISH ANCESTRY GENETIC CARRIER TESTING ACOG Committee Opinion Number 298, August 2004
Testing and screening options should be made available to all pregnant women
Prenatal Screening & Testing *First and Second Trimester Integrated and Sequential Screening
Test Performance • Detection rate – the percentage of affected that are test “positive” • (the higher, the better) • False positive rate – the percentage of unaffected that are test “positive” • (the lower, the better)
Goals in Prenatal Screening: • High sensitivity - low false positive rate • Wide availability • Reproducibility and accuracy • Human error, testing conditions
First Trimester Screening • 11-13 6/7 weeks (CRL 39-79 mm) • Maternal serum sample for PAPP-A and Free b-HCG • Ultrasound for Nuchal translucency • Detection Rates: • 80% for Trisomy 21 • 90% for Trisomy 18 • Does not screen for NTDs
Increased NT vs Cystic Hygroma • Increased NT > 95th% • With or without septations • Structural defects • Heart defects most common • Syndromic associations • Chromosomal defects • Exponential increase with increased NT • 50% Down syndrome • 25% Trisomy 13 or 18 • 10% Turner Syndrome • 5% Triploidy • 10% other NT > 3 mm is ABNORMAL
Second Trimester Serum Screening: Chromosome Abnormalities • Maternal Serum Screening • 15-20 weeks • Triple screen: 60% for T21 • Quad screen: 70% for T21 • Gestational Age Dependent** • Targeted Ultrasound • 50% aneuploid fetuses will have ultrasound markers
Prediction SURUSS 100 81% 74% 80 FASTER 66% 76% 69% 60 59% 42% DR at 5% FPR 40 37% 30% 20 0 AGE +AFP +hCG +uE3 +InhA single double triple quadruple 2nd trimester Serum Screening Test Performanceat a fixed 5% False Positive Rate(Dating by Ultrasound) Wald et al. 2000 Malone et al. 2005
Second Trimester Serum Screening: Neural Tube Defects • Neural Tube Defects • Spina Bifida • Anencephaly • AFP increased in “open” defects • Sensitivity • 90% anencephaly • 80-85% open spina bifida • False positive – 3-4%
Interpreting a Quadruple Screen Bottom Line: AFP is increased with NTDs and decreased with chromosome abnormalities
Elevated MSAFP • Incorrect Dates – most common reason • Multiples • Congenital Nephrosis • Ventral Wall Defects • IUFD • Adverse Pregnancy Outcomes • Stillbirth • Placental abruption • Preterm labor • Oligohydramnios • IUGR
Second trimester sonographic markers of Down syndrome Nuchal Fold Duodenal atresia Pyelectasis CPC Clinodactyly AV Canal
Trisomy 18Edward Syndrome • Close to 90% detected by prenatal scan • US: • Growth restriction • Clenched fists • >90% with cardiac defects • Multiple malformations • Grim prognosis • 50% Stillbirth • 50% die within the first week • 5-10% survive the first year
Trisomy 13Patau Syndrome • > 90% detected prenatally • US findings: • Midline defects including clefts, holoprosencephaly and NTDs • >90% have cardiac defects • Multiple structural abnormalities • Grim prognosis • High rate of miscarriage • 80-85% die within first month • 80-85% die within first year
Fetal Anatomy by Ultrasound • Routinely offered with prenatal care • Performed in the second trimester • 18-20 weeks optimal • Basic guidelines • Level of performance dependent upon • Who performs the scan • Where the scan is performed • Level of equipment
Gastroschisis Ventral Wall Defect Located to the Right of the Umbilicus with NO Membrane Covering Elevated MSAFP Levels Not Associated with Chromosome Abnormalities Increasing Incidence 1/10,000 >>>2-3/10,000
NTDs • Ultrasound detects 90-95% • Detection up to 98% with Ache by amniocentesis • 100% detection for anencephaly • Role of Folic Acid in Prevention: • All patients 0.4 mg per day • Previously affected 4mg per day • One month prior to conception and throughout first trimester • Decrease recurrence by up to 70%
Banana Sign Lemon Sign Meningomyelocele Sac Meningomyelocele Sac on Newborn
Pearls for Invasive Testing Risk for Sensitization Mom Rh negative – Rhogam Other antibodies may increase risk Risk for Infection transmission Hepatitis B Hepatitis C HIV Need to know familial mutations prior to performing invasive testing
Chorionic Villus Sampling • Performed 10-14 weeks • Does not test for ONTD • Technique – “Placental biopsy” • Transabdominal • Transcervical • Risk for limb reduction defects if performed < 9 weeks • Loss rate 1/100-1/200 • Risk for mosaicism (~1%)
CVS Transcervical Transabdominal Performed at 10-14 weeks
Amniocentesis > 15 weeks Loss rate 1/200 (probably closer to 1/300-1/500) Tests for ONTD Technique Fine gauge needle Ultrasound guidance Aspiration of 20-30 cc of fluid
AMNIOCENTESIS PERFORMED ROUTINELY 15-20 WEEKS Ultrasound Guided Procedure
Cordocentesis • Percutaneous Umbilical Blood Sampling • Loss rate 1/100-1/200 • Typically done after 18 weeks • Ability for: • Rapid karyotype • Blood/platelet counts • Direct fetal injections/transfusions
Fetal Blood Sampling “PUBS”
Conclusions • Many options for screening and testing. • Prenatal screening should provide the most effective test to the greatest number of women. • The best method of screening is yet to be determined. • Patient preference should be considered. • Testing and screening should be available to all women.