Download
1 / 53
540 likes | 772 Vues
The Role of Aldosterone and Aldosterone Blockade in Cardiovascular Disease. Gary E Sander, MD, PhD., FACC Professor, Tulane - New Orleans. DELETERIOUS EFFECTS OF ALDOSTERONE. DELETERIOUS EFFECTS OF ALDOSTERONE. The Contemporary View. Thrombotic Phenomena. Vascular Fibrosis.

E N D
The Role of Aldosterone and Aldosterone Blockade in Cardiovascular Disease Gary E Sander, MD, PhD., FACC Professor, Tulane - New Orleans
DELETERIOUS EFFECTSOF ALDOSTERONE DELETERIOUS EFFECTSOF ALDOSTERONE The Contemporary View Thrombotic Phenomena Vascular Fibrosis Potassium and Magnesium Loss MyocardialFibrosis Central Pressor Effects EndothelialDysfunction CatecholaminePotentiation SodiumRetention VentricularArrhythmias Cardiac and vascular damage*Hypertension, Heart Failure, Ischemia, Ventricular Dysfunction,Arrhythmia, Edema, Stroke, End-Stage Renal Disease Delyani, Exp Opin Invest Drug 1998. Zannad, Eur HeartJ 1995. Brown et al, Hypertension 1998. * In the absence of aldosterone-receptor blockade, aldosterone may cause cardiac and vascular damage.
Aldosterone Stimulates Myocardial Fibrosis in Animal Model Plasma HBP LVH Fibrosis Unilateral renal artery stenosis Angiotensin II Aldosterone Yes Yes Yes Fibrosis Aldosterone infusion in uninephric rat Angiotensin II Aldosterone Yes Yes Yes Fibrosis Infrarenal aortic banding Angiotensin II Aldosterone Yes Yes No No fibrosis HBP = high blood pressure, LVH = left ventricular hypertrophy Brilla et al, Circ Res 1990.
Aldosterone Correlates WithIncreased LV Mass 45 r=0.559 p<0.001 40 35 30 Aldosterone (ng/dL) 25 20 15 10 5 0 0 50 100 150 200 250 Left ventricular mass index (g/m2) Duprez et al, Am J Cardiol 1993.
Aldosterone Correlates WithDecreased Large-Artery Compliance 30 25 20 Plasma aldosterone (ng/dL) 15 10 r=0.795 p<0.002 5 0 0 0.5 1.0 1.5 2.0 2.5 Proximal arterial compliance (mL/mmHg) Duprez et al, Eur Heart J 1998.
The Role of Spironolactone in the Treatment of Patients with Refractory Hypertension Inclusion: • essential HTN ≥ 6 months • Clinical and mean ABP > 140/90 on ≥ 2 drugs • No prior treatment with spironolactone • No renal insufficiency • Results • after 1 month of therapy, 23/25 patients had clinical BP < 140/90 • ABPM after 1 month: 152±2/86±2 128±2/76±2 Ouzan et al Am J Hypertens 2002:15:333-9
Aldosterone levels may fall initially in response to ACE inhibition or angiotensin-II receptor blockade, but return to normal or above baseline levels (“escape”) by 12 weeks1 Multiple homeostatic mechanisms exist to preserve mineralocorticoid activity2,3 Regulators of aldosterone secretion include potassium, angiotensinII, ACTH, and other minor stimulants3 Aldosterone Synthesis Escape 1Staessen et al, J Endocrinol 1981. 2Weber, Am J Cardiol 1993. 3Zannad, Eur Heart J 1995.
Diuretic use, progressive heart failure, and death in patients in the studies of left ventricular dysfunction (SOLVD)
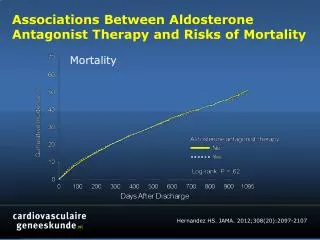
Estimated Risks, With 95% Confidence Intervals, for Patients Taking Only Non-PSDs and Those Taking PSDs Relative to the Risk of Patients Taking No Diuretics at Baseline Domanski et al JACC 2003;42:705-8.
Effect of spironolactone on cardiacsympathetic nerve activity and left ventricular remodeling in patients with dilated cardiomyopathyKasama et al JACC 2003;41:574-81
Effect Of Spironolactone On Cardiac Sympathetic Nerve Activity And Left Ventricular Remodeling In Patients With Dilated CardiomyopathyKasama et al JACC 2003;41:574-81 CONCLUSIONS Spironolactone improves cardiac sympathetic nerve activity and LV remodeling in patients with DCM
Dose-Dependent Effect of Spironolactone in Heart Failure Cicoira et al JACC 2002;40:304-10.
Dose-Dependent Effect of Spironolactone in Heart Failure Cicoira et al JACC 2002;40:304-10.
Immediate Administration of Mineralocorticoid Receptor Antagonist Spironolactone Prevents Post-Infarct Left Ventricular Remodeling Associated With Suppression of a Marker of Myocardial Collagen Synthesis in Patients With First Anterior Acute Myocardial InfarctionHayashi et al. Circulation 2003;107:2559-2565 • To evaluate the effect of mineralocorticoid receptor antagonist (MRA) spironolactone on post-infarct LV remodeling, 134 patients with first anterior acute myocardial infarction were randomly divided into the MRA (n=65) or non-MRA (n=69) groups after revascularization. • All patients were administered angiotensin-converting enzyme (ACE) inhibitor and study drug just after revascularization. • Left ventriculography with contrast medium was performed at the acute stage and after 1 month to evaluate LV remodeling. • ALD was measured at aortic root and coronary sinus. There was no difference in the baseline characteristics including infarct size and LV performance between the two groups.
Top, Changes in the LVEF, LVEDVI, LVESVI in the two randomized treatment groups from baseline to 1 month later. Bottom, Absolute change (value at 1 month-baseline) in LVEF, LVEDVI, and LVESVI. P<0.05; P<0.01; P<0.0001: difference between baseline and 1-month values (within each group). Hayashi et al. Circ 2003:107:2559-2565.
Beneficial Neurohormonal Profile Of Spironolactone In Severe Congestive Heart Failure: Results From The RALES Neurohumoral Substudy Rousseau et al JACC 2002;40:1596-1601