Download
1 / 9
90 likes | 171 Vues
Pattern of troponin ordering by ED among patients admitted to inpatient medicine. By Julia Kao UCIMC Dept of Internal Medicine 6/3/13. Objective.

E N D
Pattern of troponin ordering by ED among patients admitted to inpatient medicine By Julia Kao UCIMC Dept of Internal Medicine 6/3/13
Objective • To analyze whether troponin is being ordered appropriately by the ED for patients being admitted to internal medicine , based on chief complaint and HPI. • To determine, based on results of the analysis, whether there is potentially more cost-effective way to practice troponin ordering in the ED.
Rationale • Troponin is a marker of cardiac injury, therefore it is appropriate to order the test when there is reasonable concern for cardiac injury. • Most common clinical scenario is for patients who present with chest pain. However, substantial minority of patients present with atypical findings, e.g. dyspnea, palpitations, syncope, esp. in elderly, diabetic, and female paients. This raised concern for “under-ordering” of troponin. • Troponin frequently elevated due to reason other than cardiac injury, e.g. sepsis, renal failure, leading to concern for “over-ordering” and false positives.
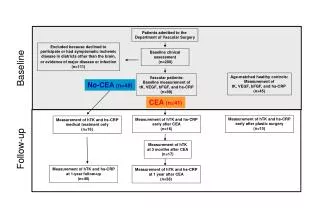
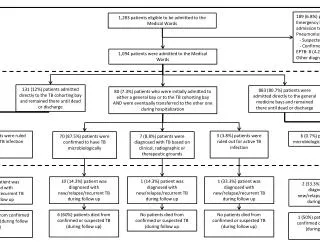
Case selection • Inclusion criteria: All ED admissions to Medicine Team A during Block 15 (4/22/13-5/12/13). • Exclusion criteria: Team A patients who were originally admitted to outside hospital or to another service, e.g. CCU/MICU. • Charts were reviewed for each patient’s chief complaint, HPI, and whether troponin was ordered by ED at admission. • For each case with troponin ordered, the case is labeled as appropriate (cardiac injury is at least of minimal concern), or inappropriate (cardiac injury not a reasonable concern) based on the CC and HPI. • For each case without a troponin at admission, case was reviewed for whether troponin should have been ordered at admission.
Results • Total number of admissions= 48 • Troponin was ordered for 24 (50%). 19 (79%) may be considered appropriate, among which 10 had chest pain, 4 had acute-onset dyspnea, 2 had acute-onset palpitations, and 3 were brought in for syncope. 5 (21%) are likely inappropriate, among which 1 had acute hepatitis, 1 had hematuria, 1 had shortness of breath due to severe ascites, 2 had orthostatic hypotension leading to recurrent dizziness. • Troponin was not ordered for 24 patients, with chief complaints ranging from UTI to chronic pancreatitis, for each case it is appropriate to defer on troponin testing.
What about cost? • Cost of troponin test= $11.08 • Excessive cost of inappropriately ordered troponin at admission for this panel of patients= $55.40 • Excessive cost of inappropriately ordered troponin multiplied by 6 medicine teams over each 3-week block= $$$$$? • Did not consider in this study: False positives may lead to additional troponins or additional cardiac testing being ordered.
Caveats of this analysis • The definition of “appropriate” ordering of troponin is generous for the analysis. • This panel of 48 patients over a random 3-week block may not be representative of the larger population of all inpatient medicine admissions to the wards. • Again, additional troponin and/or cardiac testing ordered due to positive troponin were not addressed, which may lead to higher cost, patient inconvenience, and increased length of stay.
Conclusions • The pattern of troponin-ordering by the ED for patients admitted to inpatient medicine ward suggests that there is no “under-ordering” of troponin, but there is potentially “over-ordering” of troponin (21% of the cases in this analysis) which may lead to excessive costs. • The majority of time (79% of the cases in this analysis), troponin was ordered appropriately by the ED for medicine patients admitted to wards.
References • Jaffe AS and Morrow DA. Troponins and creatinekinase as biomarkers of cardiac injury.In: UpToDate, Basow, DS (Ed), UpToDate, Waltham, MA, 2013. • Canto JG, Shlipak MG, Rogers WJ, Malmgren JA, Frederick PD, Lambrew CT, Ornato JP, Barron HV, Kiefe CI. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA. 2000;283(24):3223.