Download
1 / 71
780 likes | 1.44k Vues
Postoperative deformities of the upper lip and palate: etiology, pathogenesis, clinical features, surgical treatment of deformities. Voles of the maxillofacial area, salivary glands, etiology, symptoms, diagnosis, surgical treatment. Cleft Variants. Great anatomic variation in types of clefts!.

E N D
Postoperative deformities of the upper lip and palate: etiology, pathogenesis, clinical features, surgical treatment of deformities. Voles of the maxillofacial area, salivary glands, etiology, symptoms, diagnosis, surgical treatment.
Cleft Variants Great anatomic variation in types of clefts! Anatomic Classification based on: 1) Location 2) Completeness (Incomplete/Complete) 3) Extent Since lip, alveolus, and hard palate differ in embryologic origin, any combination can occur Clinical Aspects of Cleft Lip/Palate Reconstruction
Iowa Classification Group I Clefts of lip only Group II Clefts of palate only (2o) Group III Clefts of lip, alveolus, palate Group IV Clefts of lip and alveolus (primary cleft palate and lip) Group V Miscellaneous Clinical Aspects of Cleft Lip/Palate Reconstruction
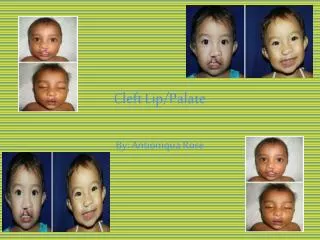
Cleft Variants Cleft Lip Expressed in structures anterior to incisive foramen - prepalatal alveolus, maxilla, lip, nasal structures Deficiency in skin, muscles, mucous membranes, maxillary/nasal bones, nasal cartilages 1) Isolated Incomplete Bilateral/Unilateral Intact skin/muscle between the lip and nose Less distortion brought on by abnormal muscle pull Gaping cleft of alveolus/lip structures to mere ‘scar’ (forme fruste) Clinical Aspects of Cleft Lip/Palate Reconstruction
2) Isolated Complete * Bilateral/Unilateral Cleft runs entire length of lip to floor of nose Abnormal muscle pull distorts nose extensively and creates wide clefts between the lip segments Clinical Aspects of Cleft Lip/Palate Reconstruction
Cleft Variants Isolated Cleft Palate Primary Palate (CL) Secondary Palate Soft Palate Hard Palate Complete/Incomplete -cleft can extend into the hard palate to any extent Clinical Aspects of Cleft Lip/Palate Reconstruction
Cleft Variants Combined Clefts Complete lip/palate Incomplete lip/palate Clinical Aspects of Cleft Lip/Palate Reconstruction
Surgical Management Cleft Lip and Palate Multidisciplinary approach Beyond lip repair are other issues: Hearing (otolaryngologists) Speech (speech pathologists) Dental (oromaxillofacial surgeons) Nutrition Psychosocial Integration with team-based approach Each case is assessed independently by those involved and a global treatment plan is instituted based on present need in his/her development Clinical Aspects of Cleft Lip/Palate Reconstruction
Surgical Management Staging and Timing of Surgery Different institutions = different practice Cleft Lip Cleft Palate Rule of 10’s IWK - 9-12 months of age Hgb = 10g Weight of 10lbs Age 10wks IWK - 6-8 weeks Clinical Aspects of Cleft Lip/Palate Reconstruction
Surgical Management Unilateral Complete Cleft Lip Goal: Symmetric shaped nostrils, nasal sill, and alar bases; well defined philtral dimple and columns; natural appearing Cupid’s bow; functional muscle repair Surgical Principle: Lengthen medial side of cleft so that it equals the vertical dimensions of non-cleft side Flap designs: 1) Triangular (Tennison-Randall) 2) Quadrangular 3) Rotation-advancement (Millard*, Mohler) Clinical Aspects of Cleft Lip/Palate Reconstruction
Millard Technique “Cut as you go” technique Preserves’ cupid’s bow and philtral dimple Scar placed in more anatomically correct position along philtral column Tension of closure under the alar base; reduces flair and promotes better molding of the underlying alveolar processes In simple medical student terms: 1) Medial flap rotates downward to achieve necessary lengthening 2) Lateral flap advances into the defect produced by downward displacement of medial flap 3) Small pennant-shaped medial flap can be used to restore nostril sill or lengthen the columella Clinical Aspects of Cleft Lip/Palate Reconstruction
In Complex Resident/Staff Terms: Clinical Aspects of Cleft Lip/Palate Reconstruction
Post-op Management Cleft Lip 1) Feedings administered with catheter tip syringe fitted with small red rubber catheter for the first 10 days post-op 2) Nipples are avoided to minimize strain on the muscle/skin sutures 3) Velcro arm restraints to protect repair from flailing hands/fingers 4) Suture line care: PRN cleansing with half strength peroxide followed with polymixin B-bacitracin ointment Clinical Aspects of Cleft Lip/Palate Reconstruction
Post-op Management Inform the parents of: Scar contracture Erythema Firmness Avoid placing in direct sunlight until the scar fully matures Clinical Aspects of Cleft Lip/Palate Reconstruction
Aesthetic vermilion-cutaneous mismatch vermilion notching tight appearing lateral lip segement lateral muscle buldge laterally displaced ala constricted appearing nostril Other dehiscence excessive scar formation Post-op Management Complications Clinical Aspects of Cleft Lip/Palate Reconstruction
Surgical Management Cleft Palate Goal: Production of a competent velopharyngeal sphincter Two most common repairs: 1) V-Y (Veau-Wardill-Kilner)* 2) von Langenbeck Main difference: V-Y repair involves elongation of the palate, while von Langenbeck does not Clinical Aspects of Cleft Lip/Palate Reconstruction
Wardill-Kilner 1) Incisions made along free margins of cleft and extend anteriorly to apex 2) Dissection continued posteriorly along oral side of alveolar ridge to retromolar trigone Clinical Aspects of Cleft Lip/Palate Reconstruction
Wardill-Kilner 3) Mucoperiosteal flaps are elevated from nasal/oral surfaces of bony palate 4) Dissection of the greater palatine vessels from the foramen lengthens the pedicle 5) Tensor veli palatini muscle is elevated off the hamulus to aid in relaxing the midline closure Clinical Aspects of Cleft Lip/Palate Reconstruction
Wardill-Kilner 6) Nasal mucosa freed from bony palate and closed to either side, or if necessary closed by using vomer flaps 7) Muscle and oral mucosa closed in a second single layer in a horizontal fashion Clinical Aspects of Cleft Lip/Palate Reconstruction
Wardill-Kilner 8) Anteriorly, the oral mucoperiosteal flaps are attached to the third flap (mucosa overlying the primary palate 9) Posteriorly, the palate is closed in 3 layers Nasal mucosa Levator muscle Oral mucosa Clinical Aspects of Cleft Lip/Palate Reconstruction
Post-op Management Cleft Palate Immediate concerns: 1) Airway management Change in nasal/oral airway dynamics 2) Analgesia Risk of oversedation and subsequent airway comprimise Acetominophen, Codeine sufficient: cont’d for 7-10 days Arm restraints to prevent placing fingers in mouth Diet restricted to liquids, soft foods (x3wks): bottles avoided Clinical Aspects of Cleft Lip/Palate Reconstruction
Post-op Management • Airway obstruction • Intraoperative bleeding • Palatal fistula • Midface abnormalities (early interventions) Complications Clinical Aspects of Cleft Lip/Palate Reconstruction
NORMAL LIP MUSCULAR ANATOMY CLEFT LIP ANATOMY
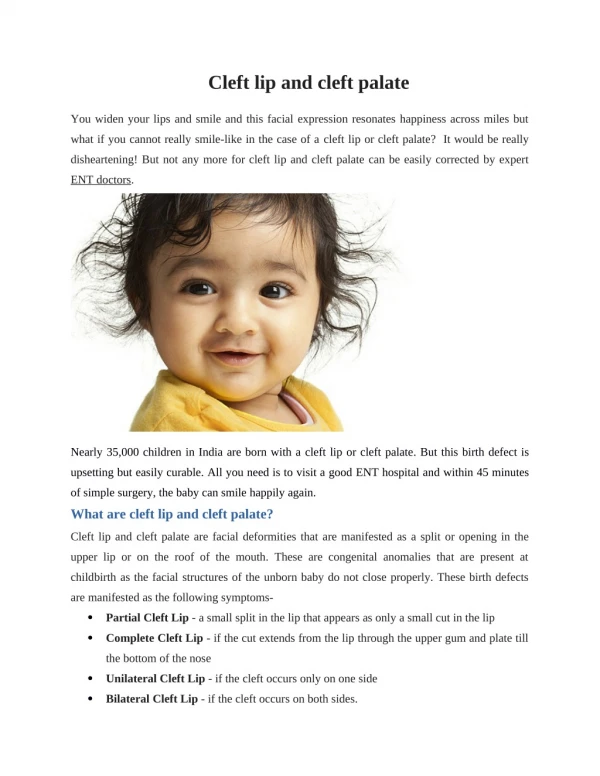
Problems in Cleft Lip and Cleft Palate • Feeding • Frequent upper respiratuary tract infection • Frequent gas regurtation • Otitis media • Nasal regurtation of food • Aspiration pneumenia • Growing retardation • Other anomalies • Psycological problems (family)
Cleft lip and palate treatment team • Surgeon experienced in cleft management • Pediatrist • Orthodontist • Pediatric Otorhinolaryngologist • Pediatric dentist • Geneticist • Spech Terapist • Social Worker • Nurse experienced in cleft problems
Feeding Rules • Swallowing is not impaired, oral feeding is possible • Bottle feed with additional cross cut in the end • Elastic plastic bottle • Bulb syringe with a nipple • Feeding with a spoon • The child should be held in a head-up position at about 45 º during and after feeding • Lateral position during sleeping
When to Operate Generally (Rules of 10’s) • Weight > 10 pound (4500 gr) • Hb > 10 gr • Age > 10 weeks Cleft lips between 3-6 months Cleft palate between 12-18 months (preferred before speech devolops)
Cleft Lip Treatment • Cleft lip • Mikroform cleft lip • Unilateral cleft lip • Bilateral cleft lip • Associated nasal deformity is classified as mild, moderate or severe • Alveolar arc position evaluated. If necessary “presurgical maksiller orthodontics” applied
Operation technique in Microform cleft (Straight line closure)
Surgical technique for unilateral cleft lip (Millard Rotation-Advancement)
Surgical technique for unilateral cleft lip (Tennison Triangular Flap)
Surgical technique for unilateral cleft lip and palate Millard techniques provides primary lip and nasal repair . It is possible “gingivoperiostoplasy” after “Presurgical maksiller ortopedics”
Pre -Orthodontic treatment After 3 months of Grayson molding plate application
A.M.Kul, right unilateral primary and secondary cleft palate Pre -Orthodontic therapy After 3 months of Grayson molding plate application