Download
1 / 65
660 likes | 1.18k Vues
Kidney Failure and Dialysis. By: Gale MacDonald and Marie Helene Bond. Presentation Overview. Kidney disease in C anada Functions of the kidney Anatomy and physiology

E N D
Kidney Failure and Dialysis By: Gale MacDonald and Marie Helene Bond
Presentation Overview • Kidney disease in Canada • Functions of the kidney • Anatomy and physiology • Kidney failure- Acute: categories; phases; causes; clinical manifestations; prevention; and nsg interventions and Chronic-stages; S/S; risk factors; prevention; nsginterventins • Screening procedures; labs test • Treatment for renal failure • Dialysis- hemodialysis and peritoneal dialysis: nursing management and equipment • Transplant- nursing management • Conservative care • Case study • Quiz • Questions
Kidney Disease in Canada • An estimated 2.6 million Canadians have kidney disease, or are at risk. • Each day, an average of 16 people are told that their kidneys have failed. • The two leading causes of kidney failure in new patients: 1. Diabetes – 35% 2. Renal Vascular Disease (including high blood pressure) – 18 %. The number of Canadians being treated for kidney failure has tripled over the past 20 years. 53% of new renal failure patients are 65 years of age or older. Among the 39,352 people being treated for kidney failure in Canada in 2010: 59% (23,188) were on dialysis 41% (16,164) had a functioning transplant.
Function of Kidneys • Production of urine and elimination of waste • Facilitates electrolyte balance • Facilitates acid-base balance • Manages water balance and maintain blood osmolality • Influences blood pressure and blood volume • Renal clearance • Secretion of prostaglandins • Conversion of vitamin D to it’s active form • Assists with red blood cell production (erythropoietin) (Day, Paul, Williams, Smeltzer, & Bare, 2010,p. 1405; Tortora & Derrickson, 2009, p. 1020 )
Urine • The formation of urine involves three major processes: • Glomerular filtration in the renal corpuscles • Tubular reabsorption • Tubular secretion
Glomerular filtration in the Renal Corpuscles • “Filtration is a process by which blood pressure forces plasma and dissolved materials out of capillaries” (Williams & Hopper, 2007, p. 752) • “The blood pressure in the glomeruli is relatively high about 55mmHg. The pressure in Bowmen’s capsule in low and its inner layer is permeable, so approx 20% to 25 %of blood that enters the glomeruli becomes renal filtrate in bowmen’s capsule” (Williams & Hopper, 2007, p. 752) • “Renal filtrate is similar to blood plasma except that there is far less protein and no blood cells present” (Williams & Hopper, 2007 , p. 752). • “The glomerular filtration rate (GFR) is the amount of renal filtrate formed by the kidneys in one minute; It averages 100 to 125mL/min” (Williams & Hopper, 2007, p. 752).
Tubular reabsorption • “Tubular reabsorption is the recovery of useful materials from the renal filtrate and their return to the blood in the peritubular capillaries” (Williams & Hopper, 2007, p. 753). • Takes place in proximal convoluted tubules, distal convoluted tubules and collecting tubules (Williams & Hopper, 2007, p. 753). • “Mechanisms of reabsorption are active transport, osmosis, diffusion, facilitated diffusion and pinocytosis” (Williams & Hopper, 2007, p. 753).
Tubular Secretion • “In tubular secretion, substances are actively secreted from the blood in the peritubular capillaries into the filtrate in the renal tubules” (Williams & Hopper, 2007, p. 753). • Ammonia, creatinine, excess water soluble vitamins, the metabolic products of medications and Hydrogen ions may be secreted into urine (Williams & Hopper, 2007).
Definition: The kidneys failure to expel wastes, maintain electrolyte balance, concentrate urine, and maintain chemicals in the bloodstream that are regulated by the kidneys (ex. Renin) (Mosby’s Dictionary of Medicine, Nursing & Health Professionals, 2006). Renal Failure Can be acute or chronic
Renal Failure Acute Renal Chronic Renal Failure Failure
“Acute renal failure (ARF) is a sudden and almost complete loss of kidney function over a period of hours to days” (Day et al., 2010, p. 1435). • Oliguria: urine output of less then 400mL /day. is the most common clinical manifestation (p.1435). • Anuria (less than 50 ml of urine a day) • Elevated BUN and creatinine • Reversible if treated promptly Acute Renal Failure
Categories of ARF • Prerenal: Hypoperfusion of the kidneys. • Intrarenal: Acute damage to kidney tissue • Postrenal: obstruction to urine flow
Phases of ARF • Initiation phase: “begins with the initial insult and ends with oliguria” • Oliguria phase:” manifested by a rise in the concentration of substances usually excreted by the kidney (urea, creatinine, uric acid, potassium and magnisium)”. • Diuresis:” gradual increase in urine output, which indicates GFR has started to recover.” • Recovery: “improvement of renal function may take 3 to 12 months. Lab values may return to normal. A permanent damage of 1% to 3% in GFR function is common, but not clinically significant” (Day et al., 2010, p, 1437)
Clinical Manifestations • Pt will appear critically ill and lethargic, and confused • Skin and mucus membranes will be dry from dehydration • drowsiness, headache, muscle twitching, and seizures. • dyspnea, crackles, tachypnea, (Day et al., 2010, p. 1436)
Prevention of ARF • Provide adequate hydration to clients at risk of dehydration. ( surgical client) • Prevent and treat shock- with blood and fluids • Treat hypotension promptly • Continually assess renal function (output, Labs) • Avoid transfusion reactions (always check two RN, and Five rights and three checks • Prevent and treat infection promptly (good catheter care) and pay special attention to wounds, burns, and other precursors to sepsis • Toxic drug effects- monitor blood levels, and ensure safe does • Day et al., 2010, p. 1437
Nursing interventions • Monitor intake and output, including all body fluids • May need to stimulate production of urine with IV fluids, diuretics. • Daily weights • Monitor lab results, CBC, BUN, creatinine, urea, e’lyles • Watch hyperkalemia symptoms: malaise, anorexia, parenthesia, or muscle weakness, EKG changes • Maintain nutrition • Mouth care – dry mucus membranes • Assess for signs of cardiac involvement- dysthymias • Skin integrity problems. Edema, itching –from toxins • Signs and symptoms of infection • May need dialysis, or continuous renal replacement therapy.
Chronic Renal failure (CRF) • Definition: “ Chronic Renal failure is a progressive, irreversible deterioration of renal function in which the body ability to maintain metabolic, fluid and electrolyte balance fails, resulting in uremia or azotemia (retention of urea and other nitrogenous waste in blood) (Day et al., 2010, p. 1440).
Stages of CRF • The normal glomerular filtration rate (GFR) is 125ml/min/1.73m2 (Day et al., 2010, p. 1440) • The stages of renal failure is determined by the GFR (Day et al., 2010, p. 1440).
Stages of CRF • Stage 1: GFR>90ml/min/1.73m2 kidney damage with normal or elevated GFR • Stage 2 : GFR = 60-89ml/min/1.73m2 mild decrease in GFR • Stage 3: GFR = 30-59ml/min/1.73m2 moderate decrease in GFR • Stage 4: GFR = 15-29ML/MIN/1.73M2 Severe decrease in GFR • Stage 5: GFR<15ml/min/1.73m2 Kidney Failure (aka end stage renal failure)
Signs & Symptoms of CRF • Ammonia-like taste in mouth or urinous breath • Edema of feet, hands, arms, face and around eyes • Hypertension • Extended neck veins • Anemia • Fatigue • Neurologic disturbances • Nausea, vomiting, and anorexia • Headaches and blurred vision
Signs & Symptoms of CRF • Pruritus • Shortness of breath • Bone and joint problems • Weakness, numbness, tremors, bone pain, and paresthesia • Urine that is cloudy, tea-coloured, or bloody • Decreased urine output or trouble urinating • Foaming of urine • Proteinuria
CRF Risk Factors • People at increased risk of developing kidney disease include people who have: • Diabetes • High blood pressure or blood vessel diseases • Glomerulonephritis and other systemic diseases • Family history of hereditary kidney disease • Certain ethnic groups such as Aboriginal, Asian, South Asian, Pacific Island, African/Caribbean and Hispanic origin
Nursing interventions CRF • Assessing fluid status • Nutrition/Diet • Patient teaching • Assess emotional status and coping strategies • Assessing for complications • Administering Medications
(Mayo clinic, 2012). Sum it up: major complications • failure can affect almost every part of your body. Potential complications may include: • Fluid retention, which could lead to swelling in your arms and legs, high blood pressure, or fluid in your lungs (pulmonary edema) • A sudden rise in potassium levels in your blood (hyperkalemia), which could impair your heart's ability to function and may be life-threatening • Heart and blood vessel disease (cardiovascular disease) • Weak bones and an increased risk of bone fractures • Anemia • Decreased sex drive or impotence • Damage to your central nervous system, which can cause difficulty concentrating, personality changes or seizures • Decreased immune response, which makes you more vulnerable to infection • Pericarditis, an inflammation of the sac-like membrane that envelops your heart (pericardium) • Pregnancy complications that carry risks for the mother and the developing fetus • Irreversible damage to your kidneys (end-stage kidney disease), eventually requiring either dialysis or a kidney transplant for survival
Diagnostic Procedures • Renal ultrasound • CT • MRI • IVP • Nephrotomogram • Renal angiogram: • Renal scan: • Renal biopsy: (Williams & Hopper, 2007)
Screening: Normal blood values to assess Kidney function • Urea 1.8 – 8.2mmol/L • Potassium 3.5 – 5.0mmol/L • Phosphate 0.8 – 1.4mmol/L • Calcium 2.0 – 2.6mmol/L • Creatinine 60 – 110umol/L (female) 70 – 120umol/L (Male) • Hemoglobin 120 – 140g/L (female) 140 – 160g/L (male) • GFR 90 – 120ml/min (1.5 – 2.0ml/sec)
Screening: Urine Testing • Creatinine clearance formula: (Volume of urine [ml/min] X Urine creatinine [MMOL/L]) Serum Creatinine (mmol/L) • As renal function decreases, creatinine clearance decreases • Day et al., 2010, pp1410
Treatment of Renal Failure Medication Proper Diet Dialysis (2 types: peritoneal & hemodialysis) Transplantation Conservation Care
Treatment of Renal Failure • Medication: Medication may be used to help maintain or improve kidney function, as well as, treat complications of renal failure (eg. Antihypertensives, kayexalate, etc.) (Day et al., 2010, pp 1442).
Diet for CRF • Low protein • Low sodium • Low potassium • Fluid restrictions • Vitamin supplements • High calorie
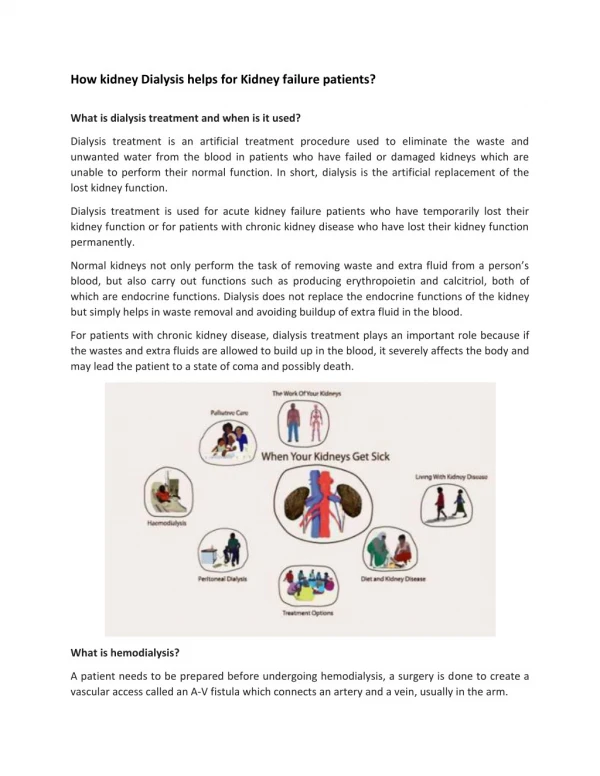
Dialysis • When the kidneys are not removing fluid and uremic waste from the body, dialysis can be used to do so • Dialysis can be acute or chronic • Acute dialysis is used for people with high levels of serum potassium, fluid overload, or impending pulmonary edema, increasing acidosis, pericarditis, and severe confusion • Acute dialysis may also be used to remove certain medications or other toxins from the blood
Dialysis • Chronic dialysis is used for chronic renal failure • Dialysis can be used for years to help maintain people with no renal function • Indications may include: uremic signs and symptoms affecting all body systems, hyperkalemia, fluid overload, pericardial friction rub, and lack of well being
Peritoneal Dialysis • Removes metabolic wastes and toxin’s so the body’s normal fluid and electrolyte balance is re-established • The peritoneum that lines the abdominal cavity and covers the abdominal organs acts as a semipermeable membrane that allows metabolic end products to be removed from the blood by means of diffusion and osmosis
Peritoneal Dialysis • An abdominal catheter allows sterile dialysate fluid to enter the peritoneal cavity • The metabolic waste products in the blood move from an area of high concentration (blood), across the peritoneal membrane, to an area of low concentration (peritoneal cavity with dialysate fluid)
Peritoneal Dialysis • The body’s excess fluid is removed by an osmotic gradient, because the dialysate fluid in the peritoneal cavity has a higher glucose concentration • the fluid is then removed from the peritoneal cavity and discarded • This process is repeated 4-6 times ever 24hrs • The most common complication from peritoneal dialysis is peritonitis
Peritoneal Dialysis • Equipment:
Peritoneal Dialysis Nursing management • Client and family education • Sterile technique (face mask, gloves, sterile field) • Signs and symptoms of peritonitis • Inspect site and dialysate solution for signs and symptoms of infection
Hemodialysis • The most common type of dialysis • Purpose remains to remove toxins from the blood and excess water from the body • Usually patients receive Hemodialysis 3 times per week • Treatment takes about 3-8 hours per treatment
Hemodialysis • The blood is delivered from the patient and to the dialysis machine, where a dialyzer (artificial kidney) uses diffusion, osmosis, and ultrafiltration to remove toxins from the blood, which is then returned to the patient • The metabolic waste products in the blood move from an area of high concentration (blood), to an area of low concentration (dialysate)
Hemodialysis • Dialysate is a solution composed of electrolytes, which concentration levels can be adjusted to accommodate the desired electrolyte level in the patients blood • Osmosis and ultrafiltration is used to remove the body’s excess water
Arteriovenous fistula- is made by sewing a vein and artery together under the skin. Fistulas may take 2 to 4 months to mature. A temporary access device is usually needed until It matures (Williams& Hopper 2007, p. 803). • Arteriovenous graft: uses a tube of systhetic material to attach an artery and a vein. Needles are inserted into the graft to access the clients blood (Williams & Hopper 2007, p. 803). Hemodialysis: Vascular Access Device