Download
1 / 48
480 likes | 489 Vues
Hypertension: A Tale of Two Worlds. Christina Lankhorst, MD FNKF September 14, 2012. Disclosures. Sanford Nephrology On NKF education committee No financial disclosures. Objectives. Define outpatient hypertension. Discuss recommendations for control.

E N D
Hypertension:A Tale of Two Worlds Christina Lankhorst, MD FNKF September 14, 2012
Disclosures • Sanford Nephrology • On NKF education committee • No financial disclosures
Objectives • Define outpatient hypertension. • Discuss recommendations for control. • Look at special cases for outpatient management (DM, CKD, elderly, etc). • Review medication classes. • Examine inpatient hypertension. • Evaluate hypertensive emergency. • Assess special cases for inpatient management (CVA, CKD, CAD).
Epidemiology • Hypertension (HTN) is common and is strongly related to cardiovascular disease. • Lowering blood pressure reduces CV disease in everyone: The ‘sicker’ and older you are, the greater the benefit from lowering BP. • If you are older (~ 60+) It’s the systolic • Nearly 1/3 of adults in the US has HTN
JNC 7 • For those patients over 50, a systolic blood pressure greater than 140 is more important to cardiovascular risk than diastolic blood pressure. • Persons who are normotensive at age 55 have a 90% lifetime risk of developing hypertension. • Starting at a blood pressure of 115/75, every increment of 20/10 leads to a doubling of cardiovascular risk. • Thiazide diuretics were the focus of initial treatment.
Appropriate Measurements of Blood Pressure • Office measurements. • Appropriate Cuff Size • Bilateral arms should be checked • Caffeine and Smoking avoided • Drug timing • Empty bladders • Five Minute rest • Good Posture • Have the cuff checked yearly • Ambulatory blood pressure monitoring. • Self-measurement of home blood pressure.
Home blood pressure monitoring (HBPM) has proven to improve patient’s adherence to medical therapy. • The target home blood pressure is less than 135/85 or 130/80 in high risk patients • HBPM can help with the diagnosis and treatment in patients with white coat hypertension and masked hypertension (BP high at home and ok in office). • It is recommended that 12 or more readings be used to make clinical decisions. Pickering et al 2008 HTN
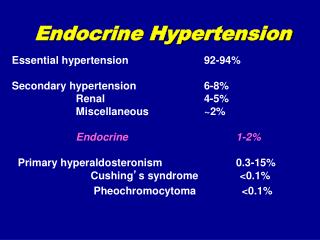
Causes of Hypertension • Essential hypertension • Sleep Apnea • Drug induced • Chronic Kidney Disease • Primary Hyperaldosteronism • Renovascular Disease • Chronic Steroid use or Cushings • Pheochromocytoma • Coarctation of the Aorta • Thyroid or Parathyroid Disease
Chronic Kidney Disease Prevalence of high BP by level of GFR, adjusted to age 60 years (NHANES III). GFR was estimated by MDRD. HTN was defined as JNC ≥ Stage 1 (SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg, or taking medications for hypertension) or JNC ≥ Stage 2 (SBP ≥ 160 or DBP ≥ 100 mm Hg). Values are adjusted to age 60 years using a polynomial regression. 95% confidence intervals are shown at selected levels of estimated GFR. K/DOQI clinical practice guidelines for chronic kidney disease: Am J Kidney Dis 39:S1-S266, 2002 (suppl 2)
Special Considerations in Selecting Drug Therapy • Coexisting diseases and therapies • Quality of Life • Physiologic and biochemical measurements. • Drug interactions • Economic considerations
How low should you go? • Clear benefits of lowering blood pressure to 140/85 mmHg; efforts to lower BP further give little benefit in NON-diabetics. • Patients with diabetes and/or renal disease: 130/80 mmHg • No trials have been done comparing different systolic targets • No evidence for lower targets, although there is supposed to be an NIH trial soon.
Compelling Indications • Coronary heart disease • Heart Failure • Diabetes • Chronic Kidney Disease • Minorities • Elderly • CVD
Hypertension in the Elderly • Isolated systolic hypertension is more common due to arterial stiffness. • White coat hypertension is more common. • Postural hypotension limits ability to treat. • Concern for interaction with other medications is frequent. • There is some evidence that lowering BP will reduce the incidence of cognitive decline and dementia. • Two of the major trials for BP in the elderly: • HYVET • SHEP
Hypertension in the Elderly • Hyvet – Hypertension in the Very Elderly • The target was 150/80 • Mortality reduce 21%, HF 64%, stroke 30% • These were pts who were healthier than typical 80+ yo patients. • Indapamide +/- perindopril • SHEP – Systolic Hypertension in the Elderly Program • Patients had to have SBP > 160 and DBP > 90 • Chlorthalidone +/- atenolol was used. • Treatment lowered the incidence of cardiovascular death by 32%, stroke 36%, HF 54%, and MI 27% Acelajado Clin Geri Med 2008
Resistant Hypertension • Failure to achieve targets on 3 drugs (including diuretic) • Older age, BMI, African American, excess sodium, alcohol • Secondary causes: aldo, sleep apnea, RVH • Excess sympathetic tone, increased aldo • Lifestyle, diuretics, aldosterone blockade
Hypertensive Emergency • Defined as marked elevation in blood pressure accompanied by acute target-organ damage. • This requires IV therapy and hospitalization. • Hypertensive Urgency usually refers to the marked elevation of blood pressure, but without target-organ damage. • Those without organ damage often do not require hospitalization, but do need more urgent adjustment of medications and follow up.
Causes of Hypertensive Emergencies • Essential Hypertension • Renal Parenchymal Disease • Renovascular Disease • Pregnancy (Eclampsia) • Endocrine (Pheo, Cushing, Renin-Secreting tumors) • Drugs • Autonomic Hyper-Reactivity (post GB syndrome) • CNS disorders
Who is at Risk • Poorly controlled blood pressure (systolic) • Tisdale • AA, Male, Poorly adherent • Shea NEJM • Pre-existing target organ damage • CVA, MI, HF, ? CKD • Tisdale
Going Forward • Is this Emergency • What “type” of presentation is it? • Main organ at risk • What do you reach for?
Treatment • Use IV route • Oral and IM route have less predictable absorption • Decide on volume status • Usual dry • Use short acting agents • Basic Tests • BMP, CBC (smear) U/A, EKG, imaging (per presentation) • Think Ahead • What will be the goal BP • Be ready to back off.
Specific Associations • Neuro – Nitroprus; Labetalol • Cardiac – NTG, NIC, NTP, Enalapril • Autonomic – Phentolamine (pheo) • Vascular – Esmolol and NTP; NIC • Renal – Fenoldepam • Obstetrical – Hydralazine; MgSO4 • Post-Op – NIC; Labet; Esmo; Clevidipine
Caveats • Look for the cause. If no evident at first, then remain vigilant. It will usually show up. • Don’t give a diuretic without a volume reason. • Follow up
Recap • Admit to a monitored bed • Use Parenteral meds • Goal BP reduction up to 25% of presenting value within 1-60 minutes • If stable after that, then aim for 160/100 mm Hg over the next 2-6 hours. • Watch for CNS or Cardiac decompensation – be prepared to back off.
Hypertension in the hospital without emergency/urgency • Just as about 1/3 of the US has hypertension, about 1/3 or more of patients in the hospital has hypertension. • There are not really many studies specifically addressing goals of treatment in the hospital. • Discharge meds vs admit meds.
Special Inpatient Cases • Stroke • Renal failure • Cardiac disease
Problems with Inpatient Pressures • Full Bladder • Pain • Dressing Changes • Stopping PO meds • Hypercapnea, Hypoglycemia • Position patient’s blood pressures are taken
Dialysis – Another World • There are limited studies on controlling blood pressure in patients on dialysis. • No consistent guidelines available due to the fact that no one knows what blood pressure to target. • Pre, Post, intradialytic, non-dialysis day.