Download
1 / 18
200 likes | 1.23k Vues
Responses to the mTOR Inhibitor Sirolimus in Patients with Malignant PEComa. Andrew Wagner , Robert Maki, Cristina Antonescu, Christopher Fletcher, Jeffrey Morgan Dana-Farber Cancer Institute, Boston Brigham and Women’s Hospital, Boston Memorial Sloan-Kettering Cancer Center, New York

E N D
Responses to the mTOR Inhibitor Sirolimus in Patients with Malignant PEComa Andrew Wagner, Robert Maki, Cristina Antonescu, Christopher Fletcher, Jeffrey Morgan Dana-Farber Cancer Institute, Boston Brigham and Women’s Hospital, Boston Memorial Sloan-Kettering Cancer Center, New York CTOS 2008, London
PEComa Family of Tumors • Lymphangioleiomyoma (LAM) • Cystic lung disease and numerous small lung nodules • Retroperitoneal masses • Angiomyolipoma (AML) • benign renal tumors • epithelioid AML = PEComa • Perivascular Epithelioid Cell tumor (PEComa) • Share common histologic appearance • Express MITF/TFE3 and melanocytic markers
LAM/AML Tuberous Sclerosis-Associated or sporadic Sabatini (2006) Nature Reviews Cancer 6:729
Sirolimus in LAM/AML 47% tumor reduction 14% Bissler et al (2008) NEJM 358:140
Case Series • Review of 3 consecutive patients with metastatic or advanced PEComa • no known effective systemic therapies • Dana-Farber Cancer Institute • Memorial Sloan-Kettering Cancer Center • Clinical management with sirolimus by treating physician
Patient 1 – Uterine PEComa 61 F with uterine bleeding in 2007 TAH - 9 cm PEComa arising from cervix Staging studies – numerous bilateral pulmonary metastases Sirolimus 4 mg, transiently increased to 8 mg but reduced to 4 mg for mild stomatitis
Patient 1 – Uterine Sarcoma Restaging at 3 months showed significant progression of disease • Sirolimus level 5 ng/mL • Dose increased to 8 mg Restaging 1 month later: further progression • Sirolimus level 7 ng/mL • Dose reduced to 2 mg and CYP450 3A4 inhibitor (clarithromycin) added; level 20 ng/mL Restaging 1 month later showed decrease/stabilization in size of disease
Patient 2 – renal PEComa 70 M with hematuria in 2001 • Radical nephrectomy – 9 cm mass • Poorly differentiated sarcomatoid variant of clear cell adenocarcinoma 2006 Local recurrence resected 2007 Right flank pain from local-regional recurrence • Sunitinib started; progression of disease after 6 weeks 2008 Pathology review at MSKCC: PEComa • Sirolimus 4 mg oral daily – diarrhea and fatigue • Dose reduced to 1 mg oral daily with improvement in symptoms. • Restaging at 6 weeks – PR • Dose reduced to 1 mg qod. Sirolimus level 5-10 ng/mL
Patient 3 – Retroperitoneal PEComa 65 M with 20 cm RP PEComa resected in 2005, complicated by preoperative tumor rupture 2007 multifocal RP recurrence resected, with further recurrence 3 months later Phase I Met inhibitor – rapid progression 2008 – started sirolimus 8 mg/d; level 36 ng/mL
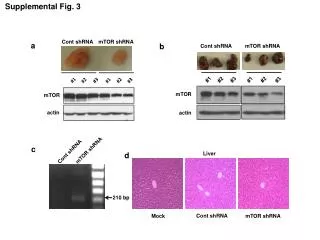
mTOR activation in malignant PEComa Sabatini (2006) Nature Reviews Cancer 6:729
phospho-S6 Immunohistochemistry Iza Malinowska and David Kwiatkowski, Brigham and Women’s Hospital
Multiplex Ligation-Dependent Probe Amplification (MLPA) Iza Malinowska, Wei Qin, David Kwiatkowski, Brigham and Women’s Hospital
Conclusions • mTOR activation, through loss of inhibition by TSC1/2 or other means, is important in growth of malignant PEComa • Potential dose-dependent effect of mTOR inhibitor • A clinical study of mTOR inhibition in malignant PEComa is warranted
DFCI Amy Potter, NP Kathy Polson, NP Bonnie Dirr, NP James Butrynski, MD Jeff Morgan, MD Suzanne George, MD George Demetri, MD Chan Raut, MD BWH Iza Malinowska, PhD Wei Qin, PhD David Kwiatkowski, MD, PhD Jason Hornick, MD, PhD Alessandra Nascimento, MD Christopher Fletcher, MD MSKCC Robert Maki, MD, PhD Cristina Antonescu, MD Ludwig Center for Cancer Research at DF/HCC SPECIAL Fund for PEComa Research The Patients and their families Thank You!