Download
1 / 1
10 likes | 124 Vues
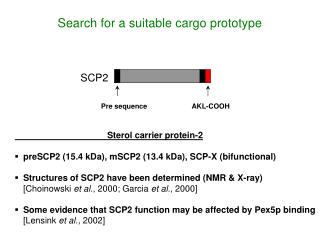
A prototype program for analyzing 4D image guidance shifts for lung SBRT Brian Wang 1 , Vikren Sarkar 1 , Christopher Busselberg 2 , Prema Rassiah-Szegedi 1 , Hui Zhao 1 , Jessica Y. Huang 1 , Martin Szegedi 1 , and Bill J. Salter 1

E N D
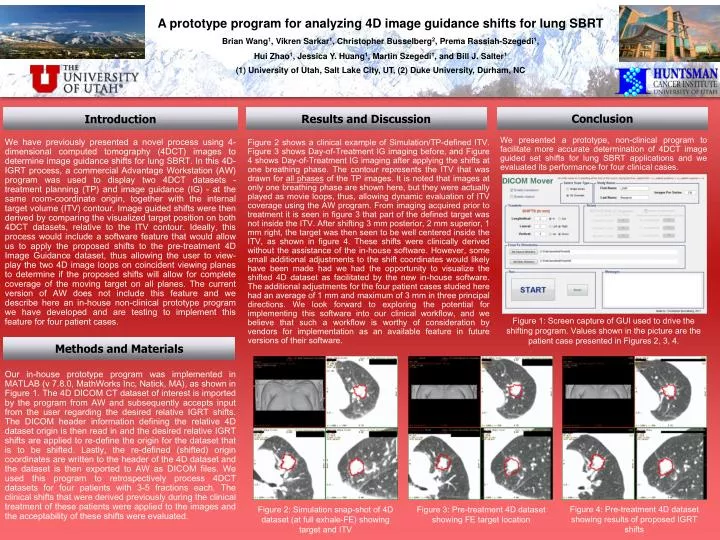
A prototype program for analyzing 4D image guidance shifts for lung SBRT Brian Wang1, Vikren Sarkar1, Christopher Busselberg2, Prema Rassiah-Szegedi1, Hui Zhao1, Jessica Y. Huang1, Martin Szegedi1, and Bill J. Salter1 (1) University of Utah, Salt Lake City, UT, (2) Duke University, Durham, NC Conclusion Results and Discussion Introduction We presented a prototype, non-clinical program to facilitate more accurate determination of 4DCT image guided set shifts for lung SBRT applications and we evaluated its performance for four clinical cases. We have previously presented a novel process using 4-dimensional computed tomography (4DCT) images to determine image guidance shifts for lung SBRT. In this 4D- IGRT process, a commercial Advantage Workstation (AW) program was used to display two 4DCT datasets - treatment planning (TP) and image guidance (IG) - at the same room-coordinate origin, together with the internal target volume (ITV) contour. Image guided shifts were then derived by comparing the visualized target position on both 4DCT datasets, relative to the ITV contour. Ideally, this process would include a software feature that would allow us to apply the proposed shifts to the pre-treatment 4D Image Guidance dataset, thus allowing the user to view-play the two 4D image loops on coincident viewing planes to determine if the proposed shifts will allow for complete coverage of the moving target on all planes. The current version of AW does not include this feature and we describe here an in-house non-clinical prototype program we have developed and are testing to implement this feature for four patient cases. Figure 2 shows a clinical example of Simulation/TP-defined ITV. Figure 3 shows Day-of-Treatment IG imaging before, and Figure 4 shows Day-of-Treatment IG imaging after applying the shifts at one breathing phase. The contour represents the ITV that was drawn for all phases of the TP images. It is noted that images at only one breathing phase are shown here, but they were actually played as movie loops, thus, allowing dynamic evaluation of ITV coverage using the AW program. From imaging acquired prior to treatment it is seen in figure 3 that part of the defined target was not inside the ITV. After shifting 3 mm posterior, 2 mm superior, 1 mm right, the target was then seen to be well centered inside the ITV, as shown in figure 4. These shifts were clinically derived without the assistance of the in-house software. However, some small additional adjustments to the shift coordinates would likely have been made had we had the opportunity to visualize the shifted 4D dataset as facilitated by the new in-house software. The additional adjustments for the four patient cases studied here had an average of 1 mm and maximum of 3 mm in three principal directions. We look forward to exploring the potential for implementing this software into our clinical workflow, and we believe that such a workflow is worthy of consideration by vendors for implementation as an available feature in future versions of their software. Figure 1: Screen capture of GUI used to drive the shifting program. Values shown in the picture are the patient case presented in Figures 2, 3, 4. Methods and Materials Our in-house prototype program was implemented in MATLAB (v 7.8.0, MathWorks Inc, Natick, MA), as shown in Figure 1. The 4D DICOM CT dataset of interest is imported by the program from AW and subsequently accepts input from the user regarding the desired relative IGRT shifts. The DICOM header information defining the relative 4D dataset origin is then read in and the desired relative IGRT shifts are applied to re-define the origin for the dataset that is to be shifted. Lastly, the re-defined (shifted) origin coordinates are written to the header of the 4D dataset and the dataset is then exported to AW as DICOM files. We used this program to retrospectively process 4DCT datasets for four patients with 3-5 fractions each. The clinical shifts that were derived previously during the clinical treatment of these patients were applied to the images and the acceptability of these shifts were evaluated. Figure 4: Pre-treatment 4D dataset showing results of proposed IGRT shifts Figure 2: Simulation snap-shot of 4D dataset (at full exhale-FE) showing target and ITV Figure 3: Pre-treatment 4D dataset showing FE target location