Download
1 / 1
10 likes | 195 Vues
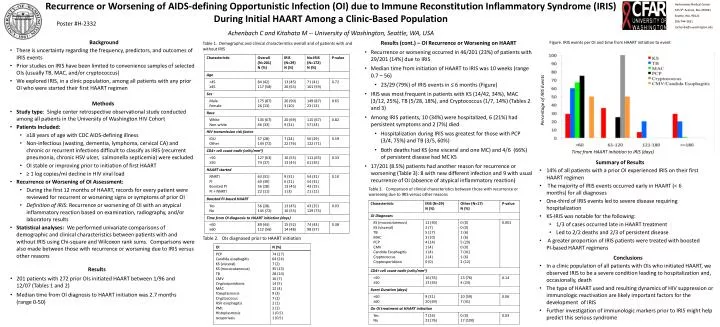
Recurrence or Worsening of AIDS-defining Opportunistic Infection (OI) due to Immune Reconstitution Inflammatory Syndrome (IRIS) During Initial HAART Among a Clinic-Based Population Achenbach C and Kitahata M -- University of Washington, Seattle, WA, USA. Harborview Medical Center

E N D
Recurrence or Worsening of AIDS-defining Opportunistic Infection (OI) due to Immune Reconstitution Inflammatory Syndrome (IRIS) During Initial HAART Among a Clinic-Based Population Achenbach C and Kitahata M -- University of Washington, Seattle, WA, USA Harborview Medical Center 325 9th Avenue, Box 359931 Seattle, WA, 98121 206-744-3631 cachenba@u.washington.edu Poster #H-2332 • Background • There is uncertainty regarding the frequency, predictors, and outcomes of IRIS events • Prior studies on IRIS have been limited to convenience samples of selected OIs (usually TB, MAC, and/or cryptococcus) • We explored IRIS, in a clinic population, among all patients with any prior OI who were started their first HAART regimen • Results (cont.) – OI Recurrence or Worsening on HAART • Recurrence or worsening occurred in 46/201 (23%) of patients with 29/201 (14%) due to IRIS • Median time from initiation of HAART to IRIS was 10 weeks (range 0.7 – 56) • 23/29 (79%) of IRIS events in ≤ 6 months (Figure) • IRIS was most frequent in patients with KS (14/42, 34%), MAC (3/12, 25%), TB (5/28, 18%), and Cryptococcus (1/7, 14%) (Tables 2 and 3) • Among IRIS patients, 10 (34%) were hospitalized, 6 (21%) had persistent symptoms and 2 (7%) died • Hospitalization during IRIS was greatest for those with PCP (3/4, 75%) and TB (3/5, 60%) • Both deaths had KS (one visceral and one MC) and 4/6 (66%) of persistent disease had MC KS • 17/201 (8.5%) patients had another reason for recurrence or worsening (Table 3): 8 with new different infection and 9 with usual recurrence of OI (absence of atypical inflammatory reaction) Figure. IRIS events per OI and time from HAART initiation to event Table 1. Demographic and clinical characteristics overall and of patients with and without IRIS Percentage of IRIS Events • Methods • Study type: Single center retrospective observational study conducted among all patients in the University of Washington HIV Cohort • Patients Included: • ≥18 years of age with CDC AIDS-defining illness • Non-infectious (wasting, dementia, lymphoma, cervical CA) and chronic or recurrent infections difficult to classify as IRIS (recurrent pneumonia, chronic HSV ulcer, salmonella septicemia) were excluded • OI stable or improving prior to initiation of first HAART • ≥ 1 log copies/ml decline in HIV viral load • Recurrence or Worsening of OI Assessment: • During the first 12 months of HAART, records for every patient were reviewed for recurrent or worsening signs or symptoms of prior OI • Definition of IRIS: Recurrence or worsening of OI with an atypical inflammatory reaction based on examination, radiography, and/or laboratory results • Statistical analyses: We performed univariate comparisons of demographic and clinical characteristics between patients with and without IRIS using Chi-square and Wilcoxon rank sums. Comparisons were also made between those with recurrence or worsening due to IRIS versus other reasons Time from HAART initiation to IRIS (days) • Summary of Results • 14% of all patients with a prior OI experienced IRIS on their first HAART regimen • The majority of IRIS events occurred early in HAART (< 6 months) for all diagnoses • One-third of IRIS events led to severe disease requiring hospitalization • KS-IRIS was notable for the following: • 1/3 of cases occurred late in HAART treatment • Led to 2/2 deaths and 2/3 of persistent disease • A greater proportion of IRIS patients were treated with boosted PI-based HAART regimens Table 3. Comparison of clinical characteristics between those with recurrence or worsening due to IRIS versus other reasons Table 2. OIs diagnosed prior to HAART initiation • Conclusions • In a clinic population of all patients with OIs who initiated HAART, we observed IRIS to be a severe condition leading to hospitalization and, occasionally, death • The type of HAART used and resulting dynamics of HIV suppression or immunologic reactivation are likely important factors for the development of IRIS • Further investigation of immunologic markers prior to IRIS might help predict this serious syndrome • Results • 201 patients with 272 prior OIs initiated HAART between 1/96 and 12/07 (Tables 1 and 2) • Median time from OI diagnosis to HAART initiation was 2.7 months (range 0-50)