Download
1 / 47
470 likes | 491 Vues
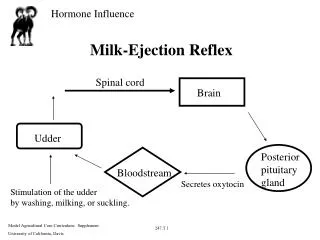
The ejection loop. Changing filling pressure changes stroke volume only by changing LVEDV. This could be an example of transfusion. Lowering LVEDP has the opposite effect (hemorrhage). Lowering the aortic pressure causes the ventricle to empty more completely.

E N D
Changing filling pressure changes stroke volume only by changing LVEDV This could be an example of transfusion Lowering LVEDP has the opposite effect (hemorrhage)
Lowering the aortic pressure causes the ventricle to empty more completely. The stroke volume increases by an amount equal to the fall in LVESV. LVEDV is not affected. Raising aortic pressure has the opposite effect
Increasing contractility decreases LVESV and thus increases stroke volume. LVEDV is not affected. Heart failure has the opposite effect
Decreasing the diastolic compliance decreases LVEDV and stroke volume but has no effect on LVESV
There are only three ways that the body regulates stroke volume from minute-to-minute: • Filling pressure (preload) • Aortic pressure (afterload) • Contractility
The real ejection loop has a rounded top since the blood pressure increases during ejection (auxotonic beat)
Decreased compliance occurs only in disease and is not a physiological regulator
T = R · P 2 The law of Laplace for a sphere:
Hypertrophy Normal Dilation
T = R · P 2 Hypertrophy results from increased afterload over several months. Hypertrophy Normal Dilation results from persistently elevated preload over several days. Dilation
T = R · P 2 Hypertrophy results from increased afterload over several months. Hypertrophy Normal Dilation results from persistently elevated preload over several days. Dilation Fiber slippage at the desmosomes will occur before the fibers will extend beyond Lo
T = R · P 2 The large chamber diameter and thin wall puts the dilated heart at a mechanical disadvantage. Hypertrophy results from increased work load over several months. Increased mass Hypertrophy Dilation results from persistently elevated preload over several days.Same mass Normal Dilation
CO = heart rate • stroke volume Theoretical CO falls dramatically at very low heart rates (< 50 b/min). Stroke volume is OK but the rate is too low Real
CO = heart rate • stroke volume Theoretical CO falls off at very high heart rates(> 180 b/min). Stroke volume decreases because diastolic filling time becomes too short. Real
CO = heart rate • stroke volume Theoretical In the normal range 50-180 b/min CO is almost independent of heart rate because cardiac output is primarily determined by the peripheral vasculature Real This is for a dog. Humans get in trouble around 140 bpm
When heart rate increases due to sympathetic stimulation (exercise) the duration of the phase 2 is shortened due to the norepinephrine which allows more time for diastolic filling than during a tachyarrhythia where ventricular action potential duration is not shortened as much. It also decreases refractory periods at the AV node. As a result you can exercise to heart rates as high as 200 b/min with no problems.
How can we measure contractility in a human heart? Ventricular function curve VMAX Ejection fraction Emax
Three factors control the stroke volume: filling pressure, aortic pressure and contractility. So how can we control for the former two?
By plotting the stroke work against filling pressure any change in filling pressure is accounted for.
Using stroke work instead of stroke volume corrects for changes in aortic pressure.
Notice that stroke volume change in a reciprocal manner. Stroke Work = P x Vol As P goes up V naturally goes down so their product remains constant. Stroke work should be independent of any change in blood pressure.
If aortic pressure is held constant stroke volume increases with contractility. Stroke volume goes down as aortic pressure goes up. Since stroke volume changes reciprocally with aortic pressure their product (stroke work) is relatively independent of aortic pressure
How can we measure contractility in a human heart? Ventricular function curve VMAX Ejection fraction Emax
Vmax The maximum velocity of shortening Vmax as calculated from the force velocity curve is independent of length and a good index of contractility. Unfortunately there is no good way to measure it in a patient. Although not used in the clinics the national board exams still ask about it.
How can we measure contractility in a human heart? Ventricular function curve VMAX Ejection fraction Emax
How can we measure contractility in the patient? Ejection fraction = (LVEDV-LVESV) / LVEDV The fraction of the ventricular contents at end diastole that is ejected.
How can we measure contractility in the patient? Ejection fraction = (LVEDV-LVESV) / LVEDV A normal ejection fraction should be above 0.50. Ejection fractions of 0.30-0.50 are of concern. Values below 0.30 carry a poor prognosis.
50-60 normal 35-49 concern <35 serious How can we measure contractility in the patient? Ejection fraction = (LVEDV-LVESV) / LVEDV • Can be easily measured by • X-ray cine • nuclear techniques • echo
Often contractility is lost in just a region of the heart as occurs in a myocardial infarction. Regional dysfunction can be seen with ultrasound or with a cine X-ray of the ventricle. Normal Regional akinesis
How can we measure contractility in a human heart? Ventricular function curve VMAX Ejection fraction Emax
dP/dV =Emax Pressure Volume Vo The heart appears to vary its elasticity from very elastic in diastole to very stiff in systole. The maximum stiffness Emax occurs during systole. Emax and Vo (volume at zero pressure) describe the ventricle.
A device called the conductance catheter allows instantaneous measurement of ventricular volume and pressure so that an ejection loop can be traced in real time in a patient. By varying aortic pressure several end-systolic pressure-volume points can be measured.
By fitting a straight line to the ESPVR, Emax and Vo cal be calculated
Clinical signs are always important indicators of reduced contractility. They include • Poor exercise tolerance • Peripheral or pulmonary edema • Elevated venous pressure • Increased cardiac size • Symptomology including orthopnea and fatigue.
The area within the ejection loop is proportional to the mechanical work done by the heart (external work).
The external work correlates poorly with the oxygen consumption (metabolic energy) of the heart.
If the triangle to the left of the ejection loop is added to the area of the ejection loop, the correlation with oxygen consumption is almost perfect. It can be shown that the triangle correlates with internal work during the isovolumetric phase of contraction.
Diastole Isovolumetric Phase Ejection shortens Internal work done as CE contracts to stretch series elastic. External work done as weight is lifted.
Increased blood pressure may cause less external work but will always increase oxygen consumption. Elevated blood pressure puts a high metabolic load on the heart.
Decreasing blood pressure will always decrease oxygen consumption.
A calcium antagonist decreases: Blood pressure Contractility Venous pressure Good anti-anginal drug!