Download
1 / 36
360 likes | 579 Vues
IMMUNOPHENOTYPE OF INFLAMMATORY CELLS OF RENAL ALLOGRAFT BIOPSIES WITH ACUTE CELLULAR REJECTION. XXVIIth International Congress of International Academy of Pathology Athens 12-17 October 2008.

E N D
IMMUNOPHENOTYPE OF INFLAMMATORY CELLS OF RENAL ALLOGRAFT BIOPSIES WITH ACUTE CELLULAR REJECTION XXVIIth International Congress of International Academy of Pathology Athens 12-17 October 2008 Mosquera Reboredo J. M1.; Vázquez Martul E.1; Fernández Rivera C.2 ; Filgueira Fernández P.3 ; and Valdés Cañedo F2. 1Pathology Deparment, 2Nephrology Deparmentand 3Investigation Laboratory.
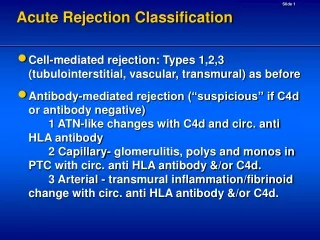
ACUTE CELLULAR REJECTION Banff 97 diagnostic categories for renal allograft biopsies—Banff’07 update 4. T-cell-mediated rejection (TCMR, may coincide with categories 2 and 5 and 6) Acute T-cell-mediated rejection (Type/Grade:) IA. Cases with significant interstitial infiltration (>25% of parenchyma affected, i2 or i3) and foci of moderate tubulitis (t2) IB. Cases with significant interstitial infiltration (>25% of parenchyma affected, i2 or i3) and foci of severe tubulitis (t3) IIA. Cases with mild-to-moderate intimal arteritis (v1) IIB. Cases with severe intimal arteritis comprising >25% of the luminal area (v2) III. Cases with ‘transmural’ arteritis and/or arterial fibrinoid change and necrosis of medial smooth muscle cells with accompanying lymphocytic inflammation (v3) Chronic active T-cell-mediated rejection ‘chronic allograft arteriopathy’ (arterial intimal fibrosis with mononuclear cell infiltration in fibrosis, formation of neo-intima) American Journal of Transplantation 2008; 8: 753–760
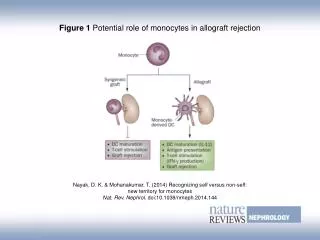
ACUTE CELLULAR REJECTION • The composition of the inflammatory infiltrate in acute rejection is dominated by T-lymphocytes (CD4 or CD8) but macrophages, plasma cell, granulocytes or NK cells can be present. • The role of T-Lymphocytes in this process is well established but not the involvement and relevance of the other inflammatory cells.
IMMUNOPHENOTYPE OF INFLAMATORY CELLS IN ACUTE CELLULAR REJECTION Rejected human renal allografts: recovery and characteristics of infiltrating cells and antibody.Tilney NLTransplantation. 1979 Nov;28(5):421-6. The relation of different inflammatory cell types to the various parenchymal components of rejecting kidney allografts. Reitamo S,Histopathology. 1980 Sep;4(5):517-32. Composition of interstitial cellular infiltrate identified by monoclonal antibodies in renal biopsies of rejecting human renal allogafts. Hancock WWet al.Transplantation. 1983 May;35(5):458-63. Renal allograft cell infiltrates associated with irreversible rejection. Sanfilippo FTransplantation. 1985 Dec;40(6):679-85. The location, as well as the number and type of cell infiltrates are critical in evaluating cellular forms of rejection
PLASMA CELLS AND AUTE CELLULAR REJECTION PLASMA CELL RICH REJECTION POOR PROGNOSIS Plasma cell-rich acute allograft rejection is associated with poor graft survival Is not a manifestation of concomitant chronic allograft nephropathy or viral infection, including posttransplant lymphoproliferative disorder. Plasma cell-rich acute renal allograft rejection Charney DA, Nadasdy T, Lo AW, Racusen LC. Tansplantation 1999: 68; 791-797 - Plasmacytic infiltrates in renal allografts comprise a spectrum of lesions from acute rejection to PTLD, with a generally poor prognosis for long-term graft survival. The clinical and pathologic implications of plasmacytic infiltrates in percutaneus renal allograft biopsies. Meehan SM et al. Hum Pathol. 2001Feb;32(2):205-15.
PLASMA CELLS AND AUTE CELLULAR REJECTION • Oedema and plasma cell-rich acute rejections (OPcR) >10% of the graft infiltrating cells. • OPcR rejections are highly resistant to therapy and portend a poor outcome, irrespective of Banff score. • Suggest that an antibody-mediated mechanism was involved in most OPcR ( 9 of 12 patients had sings suggesting antibody mediated rejection). Desvaux et al. Nephrol Dial Transplant 2004 19 933-9
PLASMA CELLS AND ACUTE REJECTION • 52% of AHR (C4d +) showed plasmacytic infiltrates ( 16% Cd4 -) ( p=0,02) • - Evidence of acute cellular with occult humoral rejection is identified in more than 40% of late AR episodes. Implications of Immunohistochemical Detection of C4d along Peritubular Capillariesin Late Acute Renal Allograft Rejection Poduval, Meehan et al. Transplantation 2005: 27:79 228-235 • Plasma Cell-rich infiltrates correlated with C4d (p = 0.0080). Acute rejection in non-compliant renal allograft recipients: a distinct morphology Lerut E. et al Clin Transplant. 2007 May-Jun;21(3):344-51.
MAST CELLS AND ACUTE CELLULAR REJECTION MAST CELLS FIBROSIS • - Mast cell were associated with allograft fibrosis in chronic rejection and chronic CsA toxicity. Might play a pathogenic role in fibrotic process. • No mast cell increase during AR in those case that progressed to chronic rejection. Close association between renal interstitialfibrosis and mast cells Important role in the development of CAN Mast cells in human allografted kidney: correlation with interstitialfibrosis. GotoEet al Clin Transplant. 2002;16 Suppl 8:7-11.
MAST CELLS AND ACUTE CELLULAR REJECTION • Correlation between number of mast cells and time since transplantation, severity of interstitialfibrosis and with interstitial oedema (all P < 0.005). • Mast cells are increased in moderate and severe A.R. compared with mild and normal kidneys. Mast cells in acute cellular rejection of human renal allografts.Lajoie Get al. Mod Pathol. 1996 Dec;9(12):1118-25., Biopsy at 100 days: Mast cells were related to decline of long-term graft function and fibrosis Toshiro Ishidaa et al,Clinical Transplantation Volume 19 Page 817 Dec 2005 Interstitial mast cell are correlated with interstitial volume, and interstitial expression of alpha-SMA. Role in the development of early interstitial fibrosis Danilewicz MMed Sci Monit. 2004 May;10(5):BR151-6. Epub 2004 Apr 28.
EOSINOPHILS AND ACUTE CELLULAR REJECTION The prognostic value of the eosinophils in acute renal allograft rejection. Weir MRTransplantation. 1986 Jun;41(6):709-12 - The increased of eosinophils in peripheral blood(p<0.01) and/or renal graft biopsy specimen (P< 0.02)is an adverse prognostic factor in acute rejection outcome. The importance of eosinophils in kidney allograft rejection. Kormendi FTransplantation. 1988 Mar;45(3):537-9. - More than 4% eosinophils in the tissue inflamatory exsudate is a specific (91%) and fairly sensitive (78%) indicator ofan severe acute rejections.
EOSINOPHILS AND ACUTE CELLULAR REJECTION EOSINOPHILS VASCULAR REJECTION -Significant interstitial graft eosinophilic infiltrate (>10% of inflamatory infiltrate) is associated with vascular rejection in the patients on high-dose immunosupression (p=0,04) Abundance of interstitial eosinophils in renal allograft is associated with vascular rejection. Meleg-Smith S et al.Transplantation 2005;79:444-450 • Tissue eosinophilia (>10 eosinophils/mm2) is associated with vascular rejection • (P= 0.02) but is not of independent prognostic significance . Banff criteria as predictors of outcome following acute renal allograft rejecction. Macdonald FI et al. Nephrol Dial Transplant. 1999 Jul;14(7):1692-7.
EOSINOPHILS AND ACUTE CELLULAR REJECTION - Eosinophilic infiltration is a negative predictor, which can indicate higher grade,more severe course of ARAR and increased resistance to an anti-rejection therapy. - Chronic rejection was seen in 25% patients of EG and in 11% in Control Group (CG) in the first year after transplantation. Biopsy eosinophilia as a predictor of renal graft dysfunction Pol Merkur Lekarski. 2006 Aug;21(122):152-5
MACROPHAGES AND ACUTE CELLULAR REJECTION Macrophages worse prognosis.poor graft survival Intraglomerular monocyte/macrophages The significance of monocytes in glomeruli of human renal transplant. Harry et alTransplantation. 37(1):70-72, January 1984. Prognosis was significantly worse during the six months after the biopsy The presence and prognostic importance of glomerular macrophage infiltration in renal allograft. Ozdemir BH. et al.Nephron 2002 Apr 90(4) 442-6 • Macrophages are associated with steroid resistance (p < 0.01). High number of interstitial macrophages are significantly related to unfavorable graft outcome(p < 0.01). Diagnostic and predictive value of an immunohistochemical profile in aymptomatic acuterejecion of renal allograft. Copin MC. Et al. Transpl Immunol. 1995 Sep;3(3):229-39.
MACROPHAGES AND ACUTE CELLULAR REJECTION - In the intimal arteritis (Banff II or III )the infiltrating cells were predominantly macrophages. T-cell were in the minority (P< 0.01) The macrophage is the predominant inflammatory cell in renal allograft intimal arteritis Matheson PJ et al Transplantation. 2005 Jun 27;79(12):1658-62. Univariate analysis shows a trend for a higher infiltration with CD8+ (P = 0.053) and CD68+(P = 0.06) cells in clinical rejection. Inflammatory factor-1+-activated macrophages (activation marker) were increased in clinical rejection(P = 0.014) Clinical rejection is distinguished from subclinical rejection by increased infiltration by a population of activated macrophagesGrimm PC et alJ Am Soc Nephrol. 1999 10(7):1582-9.
MACROPHAGES AND ACUTE REJECTION Macrophages are a part of the pathogenesis of acute humoral rejection Transplant Mac attack:Humor the macrophagesColvin K. International 2003; 63:1953 • - Glomerular and interstitial monocyte/ macrophages(MO) infiltrations closely associated with C4d+ (p<0.0001) • -Confirm the correlation of C4d+ and PMN. • Sensitivity 91% and Specificity 93% (MO/glomerulus >1 as threshold) Propose add to the histological criteria of Acute Humoral Rejection. C4d Monocytes and peritubular capillary C4d deposition in acute renal allograft rejection Magil y Tinckam K. International 2003 63: 1888
MATERIALS AND METHODS • Review 6 month post-transplant kidney biopsies with acute cellular rejection • Grade and tabulate the histological findings according Banff score. • Measure the average per high power field (hpf) of plasma cell, macrophages, mast cells, T- lymphocytes (CD4 and CD8) and eosinophils using inmunohistochemistry. • All biopsies were stained with C4d antibody by inmunohistochemistry. • Clinical parameters like HLA mismatch, cytotoxic cross-match, type of immunosupression, creatinine level, response to anti-rejection therapy and evolution of allograft were reviewed. • Identify follow-up biopsies if available. • Statistical analysis: we used SPSS statistical software. Comparisons of different data were performed with t-Student, Man-Whitney and X2 test. Kaplan-Meier: Logistic regression for survival analysis
IMMUNOPHENOTYPE OF INFLAMATORY CELLS OF RENAL ALLOGRAFT BIOPSIES WITH ACUTE CELLULAR REJECTION The aim of this study is: • Try to find relation betwen type of cells in acute rejection and: • Are really useful do it in allograft biopsies with acute rejection • Clinical parameters • Outcome and survival rates of allograft. • Response to antirejection therapy. • HLA. • Evolution to chronic rejection
RESULTS • 76 biopsies from 70 kidney transplants (51 men and 26 women) • Age: 46,34 ( 20-68). • Donor age: 43,46 ±16,91 (2-71) • Ischemic time: 21,7±5,37 (5-33) • Time to biopsy: 37,28± 48,24 days (4-180d) • Creatinine: 6,47± 2,27 (1,70-12,30) • Proteinuria: 2,04±2,36 (0-12)
BANFF GRADE 57,9% 40,8% 39,4% 26,3% 17,1% 10,5% 2,6% 2,6% Banff grade Vascular rejection • T-test: More monocyte/macrophages in vacular rejection compared with tubulo-interstitial (60,6 vs 40,6) (p=0,039) • No correlation with U-Mann Withney (p=0,09). • No correlation with other type of cells
Glomerulitis • T-test: High number of macrophages in glomerulitis group (>g1) (55,5vs 35,7) (p=0,04). • No correlation with U-Mann Withney. • No correlation with other type of cells g0 >g1 Log rank= 5,07 p=0,024
RESULTS Fibrosis T-test:more plasma cells and Cd8 lymphocytes in cases with fibrosis compared with those without (plama cell 6,2 vs 1,1, p=0,01) (Cd8 38 vs 29,2, p=0,03) No correlation with U-Mann Withney.
Nº HLA mismaches Incompatible DR > o < 1 InDR<1 In DR> 1 p • Plasma cells1,6±3 5,1±10,40,03 • Macrophages45,7±33 50,7 ±45 ns • Mast cells0,7 ±1,2 1,5 ±3 ns • CD424,1±31 17,7 ±20 ns • CD8 43,1±39 42,9±34 ns • Eosinophils1,3 ±5 0,3±0,8 ns T-Student U-Mann Whitney no correlations. Plasma cells (p=0,58)
Nº HLA mismaches Incompatible > O < 3 RESULTADOS 2 In<3 In > 3 p • Plasma cells3,8±8,1 4,1±9,9 ns • Macrophages42,3±36,2 59,1±47 0,09 • Mast Cells1,3±2,2 1,1±3,1 ns • CD423,5±27,5 14,4±18,3 ns • CD8 45,4±35 39,5±35,8 ns • Eosinophils 0,9±3,8 0,2±0,4 ns T-test U-Man Withney : No correlation with any type of cell but macrophages p=0,07
C4d • Inmunohistochemistry • Ac. Polyclonal anti-C4d.
Banff 97 diagnostic categories for renal allograft biopsies Banff’07 update Antibody-mediated changes (may coincide with categories 3, 4 and 5 and 6) Due to documentation of circulating antidonor antibody, and C4d3 or allograft pathology C4d deposition without morphologic evidence of active rejection C4d+, presence of circulating antidonor antibodies, no signs of acute or chronic TCMR or ABMR (i.e. g0, cg0, ptc0, no ptc lamination). Cases with simultaneous borderline changes or ATN are considered as indeterminate Acute antibody-mediated rejection C4d+, presence of circulating antidonor antibodies, morphologic evidence of acute tissue injury, such as (Type/Grade): I. ATN-like minimal inflammation II. Capillary and or glomerular inflammation (ptc/g >0) and/or thromboses III. Arterial—v3 Chronic active antibody-mediated rejection4 C4d+, presence of circulating antidonor antibodies, morphologic evidence of chronic tissue injury, such as glomerular double contours and/or peritubular capillary basement membrane multilayering and/or interstitial fibrosis/tubular atrophy and/or fibrous intimal thickening in arteries American Journal of Transplantation 2008; 8: 753–760
MIXED REJECTION CELULAR AND HUMORAL - Evidence of acute cellular with occult humoral rejection is identified in more than 40% of late AR episodes. Poduval, Meehan et al. Transplantation 2005: 27:79 228-235 • Halloran Ab Antidonor in 23-38% of. A.C R Transplantation 1992; 53: 550-555. Transplantation 1996; 61: 1586-1592. - Collins et al. 20-25% of Acute Rejection have Ac.Antidonor J. Am Soc. Nephrol. 1999; 10: 2208-2214. -Terasaki Ab. in 96% of Rejections Am. J. Transplant. 2003 3:6; 665-673 - Recommend C4d in all cases of acute graft failure
C4d Negative Positive Log Rank=1,15 p=0,28
C4d AND CELLULAR INFILTRATE C4d NEGATIVE POSITIVE U-MANN WITHNEY p Plasma cells 36 41 612 0,25 Macrophages 36,6 40,3 652 0,46 Mast cells 37,8 39,1 696 0,78 CD4 Lympho. 29,3 31,7 412 0,59 CD8 Lympho. 32,1 42,9 487 0,049 Eosinophils 38,1 35,9 626 0,64 U-Mann Withney
Steroid Therapy 58,4% 41,6% Yes Yes NO Steroid resistants
Corticosteroids Resistence Univariate analysis • In multivariate analysis /logistic regression adjusted for macrophages, CD4 and CD8 lymphocytes, a high number of monocyte/ macrophages /hpf is associated with steroid resistance (Odds= 1,021 (ci95% 1-1,041) p=0,04).
ALLOGRAFT SURVIVAL Univariate Analysis • In multivariate analysis /logistic regression adjusted for plasma cells, CD4 and CD8 lymphocytes, a low number of CD8 lymphocytes /hpf is associated with better allograft survival rates (Odds= 0,96 (ci95% 0,93-0,99) p=0,039).
RESULTS Time of biopsy (< o 30 days) • T-test:higher number of macrophages in biopsies < de 30 days ( 54,8 vs 32,9 ) (p=0,035) and higher number of plasma cells in biopsies > de 30 days ( 6,9 vs 2,9)(p=0,071 ) . • U Mann Whitneyhigher number of macrophages < 30 days (P=0,043) (41,7-30,4) (U Mann Whitney 417) Immunosupression • U-Mann-Withney:higher nº of CD8 before MMF (p=0,025) (39,4-28,4) U-Mann Withney 391,
CONCLUSIONS • CD8are associated with poor prognosis (univariate and multivariate analysis), steroid resistance (univariate) and C4d. • Macrophagesare associated wih steroid resistance (univariate and multivariate analysis). Number of macrophages is higher in < 30 days biopsies. • Plama cell rich rejections are associated with worse allograft survival (univariate). • High percentege of humoral rejection associated with acute cellular rejection
ACKNOWLEDGEMENTS • Eduardo Vázquez MartulPathology Department • Constantino Fernandez RiveraNephrology Department • Purificacion Filgueira and Investigation Unit