Download
1 / 33
330 likes | 490 Vues
Cognitive impairment, Epilepsy and Brain Atrophy in two families with different severities and outcomes. 1. 2. 1. 2. 2. 1 Department of Translational Medical Sciences, Section of Pediatrics University of Naples Federico II 2 CEINGE-Biotecnologie Avanzate, Department of Biochemical and

E N D
Cognitive impairment, Epilepsy and Brain Atrophy in two families with different severities and outcomes 1 2 1 2 2 1Department of Translational Medical Sciences, Section of Pediatrics University of Naples Federico II 2CEINGE-Biotecnologie Avanzate, Department of Biochemical and Medical Biotecnologies G. Cappuccio, G. Frisso, C. Cozzolino, F. Salvatore, E. Del Giudice
Family pedigree I II III 4 3 5 6 7 ANTONIO PIO TERESA ROSA
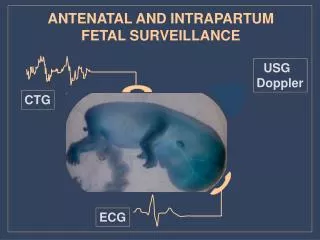
Case Report Rosa When 16 month-old seizures with loss of consciousness, lateral deviation of the head and eyes and clonic jerks lasting ten minutes, one episode per day Valproic acid, seizure improvement Hypsarrhythmia ACTH Two months later extensor type infantile spasms Lamotrigine poor response Delay in psychomotor milestones from the beginning. Loss of achieved skills such as independent ambulation. Presently she can walk with support Topiramate Good control Diffused brain atrophy
Case Report Antonio Pio Sleep EEG test At 8 months infantile spasms of the flexor type ACTH followed by Valproic Acid Severe hypotonia and delay in psychomotor milestones Uncomplete control of the spasms Recurrent episodes of apnea and comatose state Brain Atrophy Exitus
Case Report Teresa At eight months Flexor spasms Valproic acid Vigabatrin Good seizure control At 16 months recurrence of flexor spasms on awakening Sleep EEG test Topiramate seizure free Severe hypotonia and psychomotor retardation (complete head lag, unable to sit). Global brain atrophy, dismyelinization
Neuroimaging Rosa Teresa Different severity of fronto-temporal atrophy and white matter abnormalities
Neuroimaging Rosa Teresa Different degrees of brainstem and cerebellar atrophy with corpus callosum hypoplasia
Neuroimaging Teresa Rosa Vascular damages: ischemic lesions and dural ectasia with bleeding
At this point what did the biochemical and genetic exams reveal??
Investigations
Shared phenotypical and biochemical features Teresa Rosa Hyperhomocysteinemia • Epileptic encephalopaty • Microcephaly • Cognitive impairment • Brain atrophy More severe presentations Antonio Pio
Abnormal processing sample, Respiratory distress, MTHFR polimorphisms, Leukemia, Hyothyroidism, Epilepsy Hyperhomocysteinemia Methymalonic aciduria present Methymalonic aciduria absent Megaloblastic anemia absent Megaloblastic anemia present Megaloblastic anemia present Cbl Normal Cbl Low Cbl Normal/Low Met High Met Low Normal Normal TC Low TC IF deficiency IF deficiency MTHFR deficiency CBS deficiency TC TC deficiency cblC cblD cblF Normal Low cblG cblE TC deficiency
Differential Diagnosis • Remethylation defects Bishop et al., 2008; Schiff et al. 2011
Remethylation Defects MTHFR:Methylenetetrahydrofolate reductase CblE: Methionine synthase reductase CblG: Methionine synthase CBS: Cystathionine-β-synthase
Molecular analysis of MTHFR gene MTHFR gene • At 1p36.3 • Lenght 20 kb • 12 exons • mRNA 7150 bp Exons/intron and of 5’- and 3’- UTR of MTHFR gene DNA extraction from blood samples (Salting out)
Molecular analysis of MTHFR gene Direct Sequencing of PCR Products Resultsfor Teresa & parents Emilia Luigi c.547C>T (p.R183X)/ WT WT/ c.1013T>C (p.M338T) Teresa c.547C>T (p.R183X) / c.1013T>C (p.M338T)
Molecular analysis of MTHFR gene Resultsfor Rosa & parents Luisa Massimiliano Luigi p.R183X/ WT Emilia WT/ p.M338T WT/ c.1013T>C (p.M338T) c.547C>T (p.R183X)/ WT Teresa p.R183X/ p.M338T Rosa c.1013T>C (p.M338T) / c.547C>T (p.R183X)
Molecular analysis of MTHFR gene Luigi Emilia Luisa Massimiliano WT/ p.M338T p.A222V/WT p.F435F/p.F435F p.R183X/ WT p.A222V/WT p.F435F/p.F435F WT/ p.M338T p.A222V/WT p.F435F/p.F435F p.R183X/ WT p.F435F/p.F435F Teresa Rosa p.R183X/ .M338T p.A222V/WT p.F435F/p.F435F p.M338T / p.R183X p.A222V/WT p.F435F/p.F435F
Severe MTHFR Deficiency • MTHFR is the most prevalent inborn error of folate metabolism. More than 100 cases of MTHFR deficiency have been reported. • MTHFR deficiency results from the disruption of enzyme function less than 20% of controls. • Wide range of clinical manifestations from asymptomatic to severe psychomotor retardation, epilepsy, microcephaly. Sometimes central respiratory failure can be responsible for death. In the late childhood or adulthood arterial thrombosis or psychiatric disturbances can be the initial signs. • Diagnosis based on evaluation of serum Hcy and low normal level of Methionine in the absence of hemetological signs and Methylmalonicaciduria
Therapy Betaine (Cystadane)= 100-250 mg/Kg-6-9 gr/die Folinic acid (Citofolin)= 1.55 mg/kg/die B12 Vitamin (Dobetin)= 50-150 µg/die B6?? Rosa Therapy Teresa Therapy Al Tawari et al., 2002, Schiff et al., 2011, Saudubray et al. 2006
Identical genotype vs variable phenotypic expression • Previous reports described intrafamilial phenotypic variation Tonetti et al., 2001; Tallur et al., 2005; • Outcomeenviromentalmodifiers • Treatment timing • Antiepilepticdrugs (Phenytoine, Carbamazepine) Arai and Osaka, 2011, Al Essa et al., 1999, Forges e t al., 2010 - Nitrous oxide Selzer at al., 2003; • Combined defects in more • than one enzyme involved • in remethylation pathway • Different ability in Detoxification of Hcy-metabolites such as Hcy-thyolactone • Bleomycin hydrolase and Paraxonase 1 significantly contribute to Hcy-thyolactone metabolism protecting against neurodegenerationBorowczyk et al., 2012; • Age related onset of epileptic encephalopathy NEUROTOXICITY IS A MULTIFACTORIAL EVENT!
Epileptic Encephalopathy And MTHFR deficiency!!!! Epileptic Encephalopathies in Infancy and Early Childhood, 2007
Take-home messages • MTHFR deficiency is a rare entity. Infantile spasms are a possible initial manifestation. • Its important not to miss such disorders because specific and early treatment interventions are possible. The neurological outcome is more favorable earlier the treatment is administered. • Diagnostic work-up is simple and inexpensive. • Neurotoxicity in MTHFR deficiency is a multifaceted process in which the hyperhomocysteinemia may be considered a trigger and not a primary cause, increasing the susceptibility of CNS to other indipendent influences.
Merci à tout le monde The aim of medicine is to know the disease…. ..to relieve the sufferings itcauses
Rosa 12 years and 5 months Main clinical problems • Epileptic encephalopathy • Microcephaly • Severe cognitive impairment • Brain atrophy
Geni modificatori??? Identificati SNPs in geni implicati nel metabolismo dell’acido folico e della vitamina B12. Di questi, il gene ALDH1L1 (membro della famiglia aldeide deidrogenasi), si è dimostrato interagire con MTHFR
Mainclinicalproblems • Epileptic encephalopathy • Mycrocephaly • Severe cognitive impairment • Congenital hypothyroidism • Brain atrophy Exitus at 16 months 3 years and 7 months Teresa Antonio Pio • Epileptic encephalopathy • Mycrocephaly • Hypotonia • Brain atrophy • Acute respiratory distress
MTHFR deficiency • Più frequente disordine del metabolismo dei folati, AR • I polimorfismi in cis rispetto alla presenza di mutazioni patogeniche possono portare ad una riduzione dell’attività enzimatica • Neurotossicità cerebrale associata ad un aumento di Hom e riduzione die livelli di SAM Severità del fenotipo correla con la riduzione dell’attività enzimatica • I segni iniziali sono per lo più neurologici
Mutazione p.R183X in MTHFR • Mutazione nonsenso • Grave fenotipo clinico • Assenza di attività enzimatica della proteina MTHFR
Mutazione p.M338T in MTHFR • Mutazione missenso che causa alterazione del folding della proteina • Ridotta attività enzimatica della proteina MTHFR
I polimorfismi di MTHFR MTHFR p.F435F MTHFR p.A222V
Famiglia MTHFR C. Luisa WT/ p.M338T C. Massimiliano p.R183X/ WT C. Giuseppe WT/ p.M338T C. Stefania WT/ p.M338T I. Luigi p.R183X/ WT C. Emilia WT/ p.M338T C. Rosa p.R183X/ p.M338T I. Assunta WT/p.M338T I. Vincenzo WT/p.M338T I. Teresa p.R183X/ p.M338T