Download
1 / 86
1.04k likes | 2.06k Vues
Adrenergic Pharmacology. Adrenergic receptor agonists Adrenergic recpeotr antagonists. 张纬萍 浙江大学医学院药理 2012.12.3. Brain stem or spinal cord. Pre-ganglionic neuron. Ganglionic transmitter. Post-ganglionic neuron. Neuroeffector transmitter. Effector organ. Efferent neurons of ANS.

E N D
Adrenergic Pharmacology • Adrenergic receptor agonists • Adrenergic recpeotr antagonists 张纬萍 浙江大学医学院药理 2012.12.3
Brain stem or spinal cord Pre-ganglionic neuron Ganglionic transmitter Post-ganglionic neuron Neuroeffector transmitter Effector organ Efferent neurons of ANS • Neurotransmitters • Synthesis • Storage • Release • Inactivation • Receptors • Activation
Tyrosine tyrosine hydroxylase (TH)* L-DOPA DOPA decarboxylase dopamine (DA) dopamine beta-hydroxylase (DBH) norepinephrine (NE) Noradrenergic Nerve: Synthesis, storage and release of NE • Uptake • neurotransmitter transporters • uptake 1: neuronal uptake • uptake 2: non-neuronal uptake • Enzymatic degradation • monoamine oxidase (MAO) • catechol-O-methyltransferease (COMT)
Norepinephrine and Epinephrine Synthesis in the Adrenal Medulla • NE is stored in vesicles • DBH is located in vesicles • PNMT is located in the cytosol . • EPI is stored in vesicles • - EPI (~80%) and NE (~20%) released into blood • - These hormones bind adrenergic receptors on target cells, inducing the same effects as direct sympathetic nervous stimulation. PNMT NE EPI NE EPI PNMT Chromaffin cell EPI disposition: metabolism by COMT, MAO, sulfation, uptake into NE terminals
NE Metabolism - Within the same cells where the amines are synthesized, and in liver - Extraneuronal O-methylation of norepinephrine and epinephrine to metanephrines represent minor pathways of metabolism.
Norepinephrine (NE) release Act on adrenergic receptors/adrenoceptors (2 3) 1 2 1 low affinity for binding NE G-Protein Coupled Receptors
EP/NE EP/NE EP/Iso q
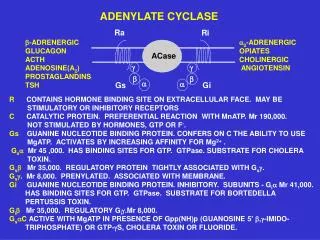
Adrenergic Receptor Subtypes & G-Protein Coupled Mechanisms a1 Adrenergic Receptors: G protein termed Gqphospholipase C activation, IP3 mechanism: mobilizes and increases intracellular free Ca2+ effects: primarily smooth muscle contraction 2 Adrenergic Receptors: Inhibition of adenylyl cyclase (AC)through Gi proteins mechanism: decreases intracellular cAMP levels effects: decreased protein phosphorylation, decreased cellular function b Adrenergic Receptors: Activation of adenylyl cyclase through Gs proteins mechanism: increases intracellular cAMP levels effects: phosphorylation of intracellular proteins smooth muscle relaxation (b2), cardiac muscle contraction (b1)
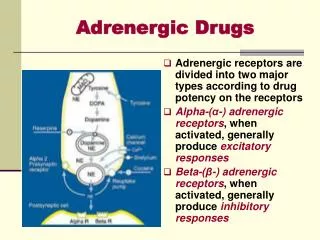
Adrenergic Receptor (adrenoreceptors) These are receptors activated by NE, EPI, or drugs with similar actions b3 fat cells (not NE)
The SNS Plays a Very Important Role in the Regulation of the Cardiovascular System, which, except for the Heart, is not Innervated by the PSNS
SNS Regulation of Cardiac Function • The SNS innervates the entire heart while the PSNS only innervates the S-A and A-V nodes. • Neural modulation of heart rate occurs in part through enhancement (NE via b1 ARs) or reduction (ACh via M2R) of pacemaker activity, which is directly stimulated by elevated cAMP levels. • The SNS via b1 ARs also increases the force of contraction. Both heart rate and contractile force contribute to cardiac output.
SNS Regulation of Blood Pressure • Acute loss of SNS function lowers blood pressure • Chronic loss of SNS function greatly increases blood pressure variability
The SNS EnhancesSmooth Muscle Contraction Primarily by a1 ARs,and Reduces ContractionPrimarily by b2 ARs
Mechanisms of drug actions 1.1 Direct actions on the receptors • Agonists • Antagonists 1.2 Indirect actions via affecting transmitters • Synthesis (L-dopa) • Transport and storage (imipramine, reserpine) • Release (ephedrine, amphetamine) • Inactivation (MAOI)
Mechanisms of drug actions 1.3 Mimetics and antagonists (1) Mimetics direct-acting: receptor agonists indirect-acting: increasing amounts and/or effects of transmitters (2) Antagonists direct-acting: receptor antagonists indirect-acting: decreasing amounts and/or effects of transmitters
Drug actions and classification Adrenoceptor agonists • , receptor agonists • epinephrine (adrenaline,肾上腺素),dopamine 多巴胺, ephedrine 麻黄碱 (2) receptor agonists • 12 receptor agonists:norepinephrine 去甲肾上腺素 • 1 receptor agonists:phenylephrine苯肾上腺素 • 2 receptor agonists:clonidine 可乐定 (3) receptor agonists: • 12 receptor agonists:isoproterenol异丙肾上腺素 • 1 receptor agonists:dobutamine 多巴酚丁胺 • 2 receptor agonists:salbutamol 沙丁胺醇
Structure-activity relationship of catecholamines and related compounds
Sympathomimetic amines • Non-catecholamine • Indirect-acting by causing the release of stored catecholamine. • Not inactivated by COMT; some are poor substrate for MAO (orally active, a prolonged duration of action) • Greater access to the CNS • Catecholamine • High potency in activating a or b receptors • Rapid inactivation by COMT and by MAO • Poor penetration into the CNS
The mode of action of sympathomimetic drugs • Direct mode • e.g. Norepinephrine • epinephrine • isoproterenol • Indirect mode • Mixed mode • e.g. ephedrine • Enhances release of stored catecholamines e.g. amphetamine • Inhibition of reuptake of released catecholamines e.g. cocaine • Inhibition of MAO e.g. pargyline
Epinephrine, Adrenaline: DIRECT Pharmacological effects 1, 2 , 1 , 2 receptor agonists (1) Cardiac effects • 1: contractility (positive inotropic), HR (positive chronotropic), cardiac output , oxygen consumption , inducing arrhythmia (2) Vascular effects (cerebral and renal circulation) • 1:vasoconstriction (skin, mucous, viscera), especially at larger doses • 2:vasodilatation of skeletal muscles and coronary vessels
Concentration-dependent response in vascular smooth muscle to epinephrine Predominant Effects low [EPI] β2 > α high [EPI] α > β2
Epinephrine, Adrenaline: DIRECT (3) Blood pressure • Systolic BP , Diastolic BP ↓(slight) (4) Respiratory • 2:dilatation of bronchial smooth muscles (Bronchodilatation) • 1:reducing congestion and edema of bronchial mucosa (5) Metabolic effects • blood glucose (hyperglycemia); free fatty acids (lipolysis)
Effects of epinephrine(therapeutic doses) systolic pressure due to increased cardiac contractile force and a rise in cardiac output . diastolic pressure usually falls due to the decrease of peripheral resistance decreasing. 1 in heart, 1 in many microvessels, 2 in the vessels of skeletal muscle
Epinephrine, Adrenaline: DIRECT (6) Smooth muscle • Effects on vascular smooth muscle are of major physiological importance. • GI smooth muscle, relax (, ) • Stomach, relax • Pyloric and ileocecal sphincters, contracted (depends on the pre-existing tone of the muscle). • Uterine, differ upon the time • Detrusor muscle(逼尿肌) of the bladder, contraction
Epinephrine, Adrenaline: DIRECT Clinical uses Systematic uses: Cardiac arrest Anaphylactic shock Acute bronchial asthma Topical uses: Adjuvant of local anesthesia Bleeding
Epinephrine, Adrenaline: DIRECT Adverse effects (1) Cardiac arrhythmias (2) Hemorrhage (cerebral or subarachnoid): reason: a marked elevation of BP (3) Central excitation:anxiety, headache... (4) Contraindications: heart diseases, hypertension, coronary arterial disease, arteriosclerosis, hyperthyroidism. Esp. patients receiving nonselective blockers.
Norepinephrine, Noradrenaline, NE: DIRECT Pharmacological effect 1, 2 receptor agonists NE and Epi are similar potent on 1 NE has little action of 2 (1) Vascular effects: 1:vasoconstriction (skin, renal, brain, hepatic, mesenteric, etc.), blood flow 2:inhibiting NE release
Actions of norepinephrine on post-synaptic (1) and pre-synaptic (2 ) receptors
Norepinephrine, Noradrenaline: DIRECT (2) Blood pressure: • Systolic BP , Diastolic BP (especially at larger doses) (3) Cardiac effects: • Weak direct stimulation (1); inhibition via reflex(in vivo) • Net result: little cardiac stimulates
Effects of catecholamines(therapeutic doses) • Predominant Effects: BP, peripheral resistance, HR • 1 receptor: vascular smooth muscle contraction • 1 receptor: myocardial contraction
Norepinephrine, Noradrenaline: DIRECT Clinical uses (limited therapeutic value) (1) Shock • used in early phase of some types of shock: small doses and shorter duration (dopamine is better; replaced by Metaraminol,间羟胺) (2) Hypotension due to drug poisoning • especially for chlorpromazine (3) Hemorrhage in upper alimentary tract,上消化道出血 • orally given after dilution
Norepinephrine, Noradrenaline: DIRECT Adverse effects (1) Ischemia and necrosis at the site of iv administrationrelieved by filtrating the area with phentolamine (receptor antagonist) (2) Acute renal failureavoiding larger doses and longer duration; monitoring urinary volume (3) Contraindicationhypertension, arteriosclerosis, heart diseases, severe urinary volume , microcirculation disorders
Dopamine: DIRECT Pharmacological effects : , receptor, dopaminergic receptor agonists (1) Cardiac effects:1 receptor, weak (2) Vascular effects: DA receptor:vasodilatation of renal and mesenteric arteries , blood flow (small doses); 1 receptor:vasoconstriction of skin, mesenteric vessels (larger doses) (3) Renal effects:renal vasodilatation; natriuretic effects
Dopamine,DIRECT Clinical uses (1) Shock, sever congestive failure • cardiac and septic shock (2) Acute renal failure • combined with furosemide Adverse effects – short-lived • tachycardia, arrhythmia, reduction in urine flow (renal vasoconstriction) L-DOPA but not dopamine can enter brain.
Isoproterenol, Isoprenaline: DIRECT 异丙肾上腺素 1 , 2 receptor agonists (1) Cardiac effects (1 receptor) (2) Vascular effects 2 receptor:dilatation of skeletal muscles and coronary vessels; SP ,DP or ,pulse pressure (3) Bronchodilatation (2 receptor) (4) Metabolism Promoting effects as epinephrine
Effects of catecholamines(therapeutic doses) Predominant Effects: HR, systolic BP, distolic BP, peripheral resistance 1, myocardial contraction 2, vascular dialization , at higher concentrations
Isoproterenol, Isoprenaline Clinical uses (1) Cardiac arrest / A-V block: in emergencies (2) Shock / Bronchial asthma: replaced by other sympathomimetics Adverse effects (1) Heart stimulation, arrhythmia (2) Contraindications:coronary heart disease, myocarditis, hyperthyroidism, pheochromocytoma.
1 receptor agonists • Heart failure (after cardiac surgery or congestive HF or acute myocardial infarction; short-term treatment) • Cardiac stimulation (-) isomer of dobutamine is a potent agonist at 1 receptors (+)-dobutamine is a potent 1 receptor antagonist Dobutamine:多巴酚丁胺,DIRECT
2 receptor agonists Terbutaline:博利康尼,DIRECT • Uses: Bronchial asthma Dilation of bronchial smooth muscle; 2 > 1 agonist (partially selective): preferential activation of pulmonary 2 receptors by inhalation. Premature Labor (combine with ritodrine,羟苄羟麻黄碱). • Adverse effects: headache, cardiac stimulation and skeletal muscle fine tremor (2 receptors on presynaptic motor terminals; their activation enhances ACh release).
Terbutaline:博利康尼 间羟异丁肾上腺素 Metaproterenol 间羟异丙肾上腺 Albuterol 舒喘灵,沙丁胺醇
2 receptor agonists Isoetharine,N-异丙基乙基降肾上腺素 Pirbuterol,吡舒喘宁吡丁醇 Bitolterol,叔丁肾上腺素双甲苯酸酯 Fenoterol,培罗坦克 Salmeterol,沙美特罗 Ritodrine,羟苄麻黄碱 Procaterol,异丙喹喘宁
1 receptor agonists Methoxamine(伐沙克新): DIRECT>INDIRECT Phenylephrine(苯肾上腺素): DIRECT>INDIRECT • Induces reflex bradycardia, used in hypotension, paroxysmal supraventricular tachycardia ; • Phenylephrine: Mydriasis(瞳孔散大), pupillary dilator muscles, no or less effect on intraocular pressure, short-acting (for several hours); act as a nasal decongestant
2 receptor agonists Clonidine(可乐定):DIRECT • Uses: antihypertensive drug; can be administered as transdermal patch (permits continuous administration) • Mechanism of action : α2-adrenergic partial agonist; actions predominantly in CNS. Lowers blood pressure by inhibiting sympathetic vasomotor tone (probably on I1 receptor). • Adverse effects: (iv administration may result in transient increase in blood pressure (activation of post-synaptic receptors); dry mouth, sedation
Other 2 receptor agonists Apraclonidine, 阿拉可乐定 Brimonidine, 溴莫尼定 Guanfacine, 氯苯乙胍 Guanabenz, 氯苄氨胍 Methyldopa, 甲多巴 Tizanidine, 替扎尼定
Ephedrine: 麻黄碱,MIXED Ephedrine Epinephrine • Promoting the release of NE, weak agonist effectson 1、2、1、2 receptors Properties: • chemically stable, orally effective; • less potent but longer action duration; • central stimulating: alertness , fatigue ↓, prevents sleep (adverse effects) • Tachyphylaxis (快速抗药反应).