Download
1 / 1
10 likes | 128 Vues
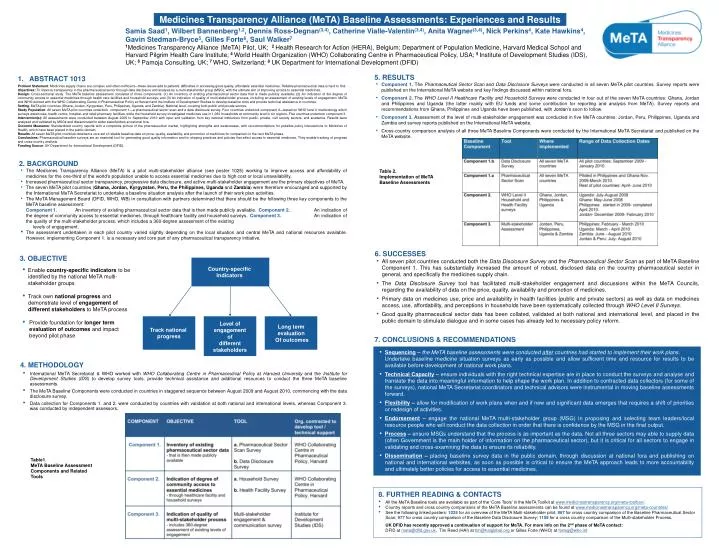
Medicines Transparency Alliance (MeTA) Baseline Assessments: Experiences and Results. Country-specific Indicators.

E N D
Medicines Transparency Alliance (MeTA) Baseline Assessments: Experiences and Results Country-specific Indicators Samia Saad1,Wilbert Bannenberg1,2, Dennis Ross-Degnan(3,4),Catherine Vialle-Valentin(3,4),Anita Wagner(3,4),NickPerkins4, Kate Hawkins4,Gavin Stedman-Bryce5, Gilles Forte6, Saul Walker7 1Medicines Transparency Alliance (MeTA) Pilot, UK; 2 Health Research for Action (HERA), Belgium; Department of Population Medicine, Harvard Medical School and Harvard Pilgrim Health Care Institute; 4 World Health Organization (WHO) Collaborating Centre in Pharmaceutical Policy, USA; 5 Institute of Development Studies (IDS), UK; 6Pamoja Consulting, UK; 7 WHO, Switzerland; 8UK Department for International Development (DFID) Track national progress Level of engagement of different stakeholders Long term evaluation Of outcomes 5. RESULTS • Component 1. The Pharmaceutical Sector Scan and Data Disclosure Surveys were conducted in all seven MeTA pilot countries. Survey reports were published on the International MeTA website and key findings discussed within national fora. • Component 2. The WHO Level II Healthcare Facility and Household Surveys were conducted in four out of the seven MeTA countries: Ghana, Jordan and Philippines and Uganda (the latter mainly with EU funds and some contribution for reporting and analysis from MeTA). Survey reports and recommendations from Ghana, Philippines and Uganda have been published, with Jordan’s soon to follow. • Component 3. Assessment of the level of multi-stakeholder engagement was conducted in five MeTA countries: Jordan, Peru, Philippines, Uganda and Zambia and survey reports published on the International MeTA website. • Cross-country comparison analysis of all three MeTA Baseline Components were conducted by the International MeTA Secretariat and published on the MeTA website. ABSTRACT 1013 Problem Statement: Medicines supply chains are complex and often inefficient—these issues add to patients’ difficulties in accessing good quality, affordable essential medicines. Reliable pharmaceutical data is hard to find. Objectives: To improve transparency in the pharmaceutical sector through data disclosure and analysis by a multi-stakeholder group (MSG), with the ultimate aim of improving access to essential medicines. Design: Cross-sectional study. The MeTA baseline assessment consisted of three components: (1) An inventory of existing pharmaceutical sector data that is made publicly available; (2) An indication of the degree of community access to essential medicines through health care facilities and household surveys; and (3) An indication of quality of multi-stakeholder process, including an assessment of existing levels of engagement. MeTA and WHO worked with the WHO Collaborating Centre in Pharmaceutical Policy at Harvard and the Institute of Development Studies to develop baseline tools and provide technical assistance to countries. Setting: MeTA pilot countries (Ghana, Jordan, Kyrgyzstan, Peru, Philippines, Uganda, and Zambia). National level, covering both public and private sectors. Study Population: All seven MeTA pilot countries undertook component 1—a pharmaceutical sector scan and a data disclosure survey. Four countries undertook component 2—based on WHO level II methodology which surveys warehouse, health centre, hospital, and retail pharmacy facilities, while the household survey investigated medicines use in 1,080 households at community level in six regions. Five countries undertook component 3. Intervention(s): All assessments were conducted between August 2009 to September 2010 with input and validation from key national institutions from public, private, civil society sectors, and academia. Results were analysed and validated by MSGs and disseminated to wider stakeholders at national fora. Outcome Measures: Standardized country reports with a composite picture of the pharmaceutical market, highlighting strengths and weaknesses, with recommendations for possible policy interventions to Ministries of Health, which have been placed in the public domain. Results: All seven MeTA pilot countries obtained a core set of reliable baseline data on price, quality, availability, and promotion of medicines for comparison in the next MeTA phase. Conclusions: Pharmaceutical baseline surveys are an essential tool for generating good quality information and for shaping practices and policies that affect access to essential medicines. They enable tracking of progress and cross-country analysis. Funding Source: UK Department for International Development (DFID). 2. BACKGROUND • The Medicines Transparency Alliance (MeTA) is a pilot multi-stakeholder alliance (see poster 1025) working to improve access and affordability of medicines for the one-third of the world’s population unable to access essential medicines due to high cost or local unavailability. • Increased pharmaceutical sector transparency, progressive data disclosure, and active multi-stakeholder engagement are the primary objectives of MeTA. • The seven MeTA pilot countries (Ghana, Jordan, Kyrgyzstan, Peru, the Philippines, Uganda and Zambia) were therefore encouraged and supported by the International MeTA Secretariat to undertake a baseline situation analysis after the launch of their work plan activities. • The MeTA Management Board (DFID, WHO, WB) in consultation with partners determined that there should be the following three key components to the MeTA baseline assessment: • Component 1. An inventory of existing pharmaceutical sector data that is then made publicly available. Component 2. An indication of the degree of community access to essential medicines, through healthcare facility and household surveys. Component 3. An indication of the quality of the multi-stakeholder process, which includes a 360-degree assessment of the existing levels of engagement. • The assessment undertaken in each pilot country varied slightly depending on the local situation and central MeTA and national resources available. However, implementing Component 1. is a necessary and core part of any pharmaceutical transparency initiative. Table 2. Implementation of MeTA Baseline Assessments 6. SUCCESSES • All seven pilot countries conducted both the Data Disclosure Survey and the Pharmaceutical Sector Scan as part of MeTA Baseline Component 1. This has substantially increased the amount of robust, disclosed data on the country pharmaceutical sector in general, and specifically the medicines supply chain. • The Data Disclosure Survey tool has facilitated multi-stakeholder engagement and discussions within the MeTA Councils, regarding the availability of data on the price, quality, availability and promotion of medicines. • Primary data on medicines use, price and availability in health facilities (public and private sectors) as well as data on medicines access, use, affordability, and perceptions in households have been systematically collected through WHO Level II Surveys. • Good quality pharmaceutical sector data has been collated, validated at both national and international level, and placed in the public domain to stimulate dialogue and in some cases has already led to necessary policy reform. 3. OBJECTIVE • Enable country-specific indicators to be identified by the national MeTA multi-stakeholder groups • Track own national progress and demonstrate level of engagement of different stakeholders to MeTA process • Provide foundation for longer term evaluation of outcomes and impact beyond pilot phase 7. CONCLUSIONS & RECOMMENDATIONS • Sequencing – the MeTA baseline assessments were conducted after countries had started to implement their work plans. • Undertake baseline medicine situation surveys as early as possible and allow sufficient time and resource for results to be available before development of national work plans. • Technical Capacity– ensure individuals with the right technical expertise are in place to conduct the surveys and analyse and translate the data into meaningful information to help shape the work plan. In addition to contracted data collectors (for some of the surveys), national MeTA Secretariat coordinators and technical advisors were instrumental in moving baseline assessments forward. • Flexibility– allow for modification of work plans when and if new and significant data emerges that requires a shift of priorities or redesign of activities. • Endorsement– engage the national MeTA multi-stakeholder group (MSG) in proposing and selecting team leaders/local resource people who will conduct the data collection in order that there is confidence by the MSG in the final output. • Process – ensure MSGs understand that the process is as important as the data. Not all three sectors may able to supply data (often Government is the main holder of information on the pharmaceutical sector), but it is critical for all sectors to engage in validating and cross-examining the data to ensure its reliability. • Dissemination– placing baseline survey data in the public domain, through discussion at national fora and publishing on national and international websites, as soon as possible is critical to ensure the MeTA approach leads to more accountability and ultimately better policies for access to essential medicines. 4. METHODOLOGY • International MeTA Secretariat & WHO worked with WHO Collaborating Centre in Pharmaceutical Policy at Harvard University and the Institute for Development Studies (IDS) to develop survey tools, provide technical assistance and additional resources to conduct the three MeTA baseline assessments. • The MeTA Baseline Components were conducted in countries in staggered sequence between August 2009 and August 2010, commencing with the data disclosure survey. • Data collection for Components 1. and 2. were conducted by countries with validation at both national and international levels, whereas Component 3. was conducted by independent assessors. Table1. MeTA Baseline Assessment Components and Related Tools 8. FURTHER READING & CONTACTS • All the MeTA Baseline tools are available as part of the ‘Core Tools’ in the MeTAToolkit at www.medicinestransparency.org/meta-toolbox/. • Country reports and cross country comparisons of the MeTA Baseline assessments can be found at www.medicinestransparency.org/meta-countries/ • See the following linked posters: 1025 for an overview of the MeTA Multi-stakeholder pilot; 967 for cross country comparison of the Baseline Pharmaceutical Sector Scan; 977 for cross country comparison of the Baseline Data Disclosure Survey; 1108 for a cross country comparison of the Multi-stakeholder Process. • UK DFID has recently approved a continuation of support for MeTA. For more info on the 2nd phase of MeTA contact: • DFID at meta@dfid.gov.uk, Tim Reed (HAI) at tim@haiglobal.org or Gilles Forte (WHO) at forteg@who.int