Download
1 / 19
450 likes | 2.34k Vues
This is a suppurative necrosis of lung parenchyma due to nonspecific bacterial infection. Lung Abscess. It is either primary. Or secondary on top of a preexisting lung tumour. It is usually the result of soil and seed concept.

E N D
This is a suppurative necrosis of lung parenchyma due to nonspecific bacterial infection. Lung Abscess • It is either primary. • Or secondary on top of a preexisting lung tumour. It is usually the result of soil and seed concept. • When the soil “bronchopulmonary” is compromised by chronic disease and bad defense, the clearing mechanisms are disrupted and the following means bring the invading organism (seed) to implant and invade: 1- Aspiration of infected material (e.g., during oral surgery) 2- Suppression of cough reflex (e.g, in coma or under drugs) 3- Bronchial obstruction (e.g., post -operative atelectasis, foreign body, or neoplasms 4- Pneumonia,especially bacterial 5- Ischaemia (e.g., following pulmonary infarction) 6- Septicaemia (especially staphylococcal).
The usual location is the superior segment of the lower lobe or the lower portion of the upper lobe most commonly in the right lung. Pathology: • Trapping of infected material by bronchial obstruction, sluggish clearing mechanism and ischaemia result in cell death (necrosis). Infection with pyogenic or anaerobic bacteria in any of these situations causes a lung abscess. • With excess septic and cellular exudate, a progressing edge results in cavitation and liquefaction. Pus and cellular debris fill the area. • Granulation in the wall is fibrosed and epithelialization by metaplastic squamous epithelial cells follows the partial evacuation of the necrotic contents in the surrounding bronchioles.
A) Clinical features Symptoms Diagnosis: • The onset may be abrupt or gradual. • Symptoms include fever, sweating, cough and chest pain simulating pneumonia. • The cough is often non productive at first or may produce mucoid or mucopurulent expectorate from bronchial inflammation close to the abscess area and sometimes there is blood streaking. • There is an expectoration of foul-smelling brown or gray sputum (in anaerobic organisms) or green or yellow sputum (being moist and having an ill flavor. • If this happens suddenly in large quantities, this denotes a rupture of the abscess cavity into the bronchus and blood streaking is common. • Pleural pain, especially with coughing is common because the abscess is near to the pleura.
Signs • May be minimal. Consolidation due to pneumonia surrounding the abscess is the most frequent finding. • Inspiratory rales and pleural rub may be heard. • Rupture into the pleural space produces signs of effusion or hydropneumothorax. Weight loss, anaemia, and clubbing or pulmonary osteoarthropathy appear when the abscess becomes chronic (8-12 weeks after onset). B) Chest X-ray • A dense shadow is the initial finding before rupture. • Later this opacity develops a cavity with fluid level. • Chest films may also reveal associated primary lesions, e.g., a bronchogenic carcinoma.
C) Laboratory Sputum • Stain and culture help in the identification of the organism and in designating an antibiotic therapy. • An anaerobic culture is indicated if there is a foul smelling pus. • AFBshould be sought in upper lobe lesions and chronic abscesses. Blood smear Leucocytosis (30.000/mm3) D) Bronchoscopy • Improves drainage by suctioning bronchial exudate and removing foreign bodies. • The possibility of a bronchial tumor being present should be investigated because 10% of lung abscesses are secondary to bronchogenic carcinomas.
Differential diagnosis: Pulmonary cavitation • Tuberculosis, bronchogenic carcinoma, mycosis, and staphylococcal pneumonia. Malignant abscesses • Usually result secondary to accumulation of septic material in necrotized vacuoles in a solid tumour. • The tumour usually has an irregular outline and scalloped interior, possibly with an uneven fluid level. • Sings of local infiltration such as a punch of lymphatics toward the hilum, hilar lymphadenopathy, or pressure and invasion symptoms, e.g., eaten up rib or nerve affection are frequently detected. Haematogenous lung abscesses • These usually result from septic pulmonary emboli. • Staphylococcus organisms are the dominant bacteria with other usual organisms from the respiratory flora.
Treatment: • This involves postural and bronchoscopic drainage. • Drug treatment involves intensive antimicrobial therapy that is necessary to prevent further lung destruction. • Penicillin G in big doses is the drug of choice with which to start. Initially two million units every six hours parenterally are given. This is achieved through the identification of the organism by culture and selection of the proper antibiotic using an antibiogram. • Metronidazole 300 mg four times daily for anaerobic organisms. Surgical resections May be indicated in specific chronic situations, e.g., the site of serious haemoptysis or failed medical treatment to control infection and toxaemia.
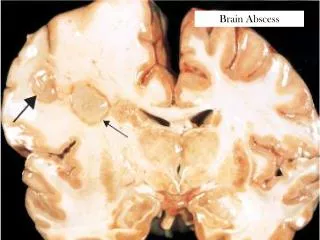
Complications • Prolonged toxaemia and chronicity with fever, pleural pain and sweating. • Severe and fatal haemorrhage. • Metastatic brain abscess. • Amyloidosis in case of prolonged suppuration. Empyema due to rupture in pleural space.
Bronchiectasis: Aetiology and pathogenesis • Bronchiectasis, the term used to describe abnormal dilatation of the bronchi • It may be acquired, or less commonly, congenital.
CAUSES OF BRONCHIECTASIS Congenital Acquired - children • Ciliary dysfunction syndromes, cystic fibrosis, primary hypogammaglobulinaemia. Acquired - adults Pneumonia (whooping cough and measles), primary tuberculosis, foreign body. • Suppurative pneumonia, pulmonary tuberculosis, pulmonary eosinophilia, bronchial tumours. • Ciliary dysfunction syndromes Primary ciliary dyskinesia (immotile cilia syndrome), Kartagener’s syndrome, Young’s syndrome.
Bronchiectasis is usually secondary to severe bacterial infection in childhood, often as a complication of whooping cough or measles. Such as a- A tuberculous hilar lymph node. b- An inhaled foreign body. Bronchiectasis may be due to bronchial distension resulting from the accumulation of pus beyond a lesion obstructing a major bronchus c- A bronchial carcinoma. • Recurrent infection and chronic obstruction by viscid mucus are both factors in causing bronchiectasis • Rarely, it may be the result of congenital dysfunction of the cilia,which is a feature of, for example, Kartagener’s syndrome (bronchiectasis, sinusitis and transposition of the viscera).
Pathology • The bronchiectatic cavities may be lined by granulation tissue, squamous epithelium or normal ciliated epithelium. • There may also be inflammatory changes in the deeper layers of the bronchial wall and hypertrophy of the bronchial arteries. • Chronic inflammatory and fibrotic changes are usually found in the surrounding lung tissue. There are three varieties 1- Cystic 2- Saccular 3- cylindrical (fusiform)
Clinical features Bronchiectasis may involve any part of the lungs but the more efficient drainage by gravity of the upper lobes usually produces less serious symptoms and complications than when bronchiectasis involves the lower lobe. The three groups of clinical features that occur in more severe cases are:
SYMPTOMS OF BRONCHIECTASIS Due to accumulation of pus in dilated bronchi Haemoptysis • Chronic productive cough usually worse in mornings and often brought on by changes of posture. Sputum often copious and persistently purulent in advanced disease. Due to inflammatory changes in lung and pleura surrounding dilated bronchi • Fever, malaise and increased cough and sputum volume when spread of infection causes penumonia, which is frequently associated with pleurisy. Recurrent pleurisy in the same site often occurs in bronchiectasis. Can be slight or massive and is often recurrent. Usually associated with purulent sputum or an increase in sputum purulence. Can, however, be the only symptom in so-called “dry bronchiectasis” General health • When disease is extensive and sputum persistently purulent a decline in general health occurs with weight loss, anorexia, lassitude, sleep sweating, and failure to thrive in children. In these patients digital clubbing is common.
Physical signs in the chest may be unilateral or bilateral and are usually basal. • In the presence of large amounts of secretion numerous coarse crepitations will be heard over the affected areas. If the bronchiectatic cavities are dry without lobar collapse there may be no abnormal physical signs. • When collapse is present the character of the physical signs depends on whether or not the proximal bronchi supplying the collapsed lobe are patent.
Bacteriological and mycological examination of sputum: Investigations • This is necessary in all patients but is especially important in bronchiectasis. Radiological examination: • Bronchiectasis, unless very gross, is not usually apparent on the conventional chest radiograph. • In advanced disease the cystic bronchiectatic spaces may be visible. • Abnormalities produced by associated pulmonary infection and/or collapse are evident. • A diagnosis of bronchiectasis can only be made with certainty by computed tomography or bronchography.
Postural drainage • The aim of this measure is to keep the dilated bronchi emptied of secretions. Management • Efficiently performed it is of great value both in reducing the amount of cough and sputum and in preventing recurrent episodes of bronchopulmonary infection. • In its simplest form, postural drainage consists of adopting a position in which the lobe to be drained is uppermost, thereby allowing secretions in the dilated bronchi to gravitate towards the trachea from which they can readily be cleared by vigorous coughing. • Percussion of the chest wall with cupped hands aids dislodgement of sputum, and a number of mechanical devices are available which cause the chest wall to oscillate, thus achieving the same effect as postural percussion and chest wall compression. • The optimum duration and and frequency of postural drainage depends on the amount of sputum but 5-10 minutes once or twice daily is a minimum for most patient.
Antibiotic therapy • Oral ciprofloxacin (250-750mg twice daily) or ceftazidime by intravenous injection or infusion (100-150 mg/kg daily in 3 divided doses). Surgical treatment • It is essential to demonstrate exactly the extent of bronchiectasis by CT scanning (or bronchography if CT is not available). • The pulmonary function must also be carefully assessed Secondary infection with bacteria such as staphylococi and Gram-negative bacilli, in particular pseudomonas species. • The most suitable cases for pulmonary resection are young patients in whom bronchiectasis is unilateral and confined to a single lobe or segment. • Unfortunately, many of the patients in whom medical treatment proves unsuccessful are also unsuitable for pulmonary resection either because of extensive bronchiectasis or co-existing chronic bronchitis. • Resection of areas of bronchiectatic lung has no role in the management of the progressive forms of bronchiectasis.
Prognosis • In many patients the prognosis is relatively good if postural drainage is performed regularly and antibiotics are used judiciously. Prevention The disease is progressive when associated with ciliary dysfunction and cystic fibrosis and inevitably causes respiratory failure and right ventricular failure. • Because bronchiectasis commonly starts in childhood following measles, whooping cough or a primary tuberculous infection, it is essential that these conditions receive adequate prophylaxis and treatment. • The early recognition and treatment of bronchial obstruction is particularly important.