Download
1 / 7
80 likes | 519 Vues
Shoulder and Elbow Assessment. Sarah Rayner ESP Physiotherapist Dr Tim Hughes GPSI MSK Orthopaedic Services. History.

E N D
Shoulder and Elbow Assessment Sarah Rayner ESP Physiotherapist Dr Tim Hughes GPSI MSK Orthopaedic Services
History Consider at baseline: age, general health and co-morbidities, nature/mechanism of onset (trauma?), pain distribution, pain behaviour (e.g. night pain, inability to lie on affected side, dead arm syndrome, catching), aggravating/easing (e.g. overhead activities), stiffness, weakness, paraesthesia, joint sounds, functional impairments and previous treatments. Frozen shoulder Primary GHJ osteoarthritis Secondary GHJ osteoarthritis ACJ osteoarthritis SCJ osteoarthritis Joint laxity Subacromial impingement Internal impingement SLAP lesion Bursitis Tendinosis Rotator cuff tear Spinal accessory neuritis Suprascapular neuritis Long thoracic neuritis Parsonage-Turner syndrome Anterior instability Anterior dislocation Multidirectional instability Posterior dislocation Fracture ACJ injury Neoplasm Referred pain from neck Referred pain from viscera
History Consider at baseline: age, general health and co-morbidities, nature/mechanism of onset (trauma?), pain distribution, pain behaviour (e.g. night pain, inability to lie on affected side, dead arm syndrome, catching), aggravating/easing (e.g. overhead activities), stiffness, weakness, paraesthesia, joint sounds, functional impairments and previous treatments. Frozen shoulder Primary GHJ osteoarthritis Secondary GHJ osteoarthritis ACJ osteoarthritis SCJ osteoarthritis Joint laxity Subacromial impingement Internal impingement Recurrence likelier in younger individuals; primary injury often causes cuff tears in the older Young adults SLAP lesion Bursitis Tendinosis Rotator cuff tear Spinal accessory neuritis Suprascapular neuritis Long thoracic neuritis Parsonage-Turner syndrome Anterior instability Anterior dislocation Multidirectional instability Posterior dislocation Fracture ACJ injury Neoplasm Referred pain from neck Referred pain from viscera >45 <40 >60 >25 >45 >40 Young adults <40 >35 <30
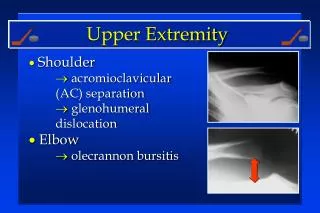
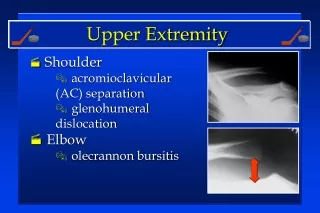
Shoulder: Common conditions • Impingement • Rotator Cuff tears • Frozen shoulder • AC joint pain
Standard tests Observations Deformity, wasting, heat, effusion, winging, bony contours Active movements Neck x 6(flex, ext, side flex and rot) Shoulder girdle elevation (SCJ, ACJ) Shoulder elevation (plus passive over-pressure) Does the movement look “right”? Is active range full? If not: Is the joint stiff? If the joint isn’t stiff, lost range may be due to weakness or pain. Painful arc? (impingement) Apley scratch test: hand down neck & hand up back (evaluate function) Passive movements Lateral rotation* (capsular pattern) Isometric actions Resisted tests Abduction Adduction Lateral Rotation Medial Rotation Rotator cuff tests Full can test (supraspinatus) Drop sign (Massive RC tear) ER lag sign (supraspinatus) Lift off test /Belly press(subscapularis) Accessory tests (as required) Scalf Test (ACJ) Neer, Hawkins and Kennedy (impingement) Palpation for tenderness As required Shoulder Assessment • * Restriction = summary of Cyriax’s “capsular pattern”
Standard tests Observations Deformity, wasting, heat, effusion, bony contours Active movements Neck x 6(flex, ext, side flex and rot) Shoulder (elevation, HBB, LR) Elbow: flex/ext, pronation/supination Wrist: flex/ext, RD/UD Is active range full? If not: Is the joint stiff? If the joint isn’t stiff, lost range may be due to weakness or pain. Passive movements End feel, crepitus, pain Isometric actions Screening tests Extension Flexion Passive stretching Combined elbow ext, wrist flex and pronation (stretches extensors) Combined elbow ext, wrist ext and supination (stretches flexors) Accessory tests (as required) Palpation for tenderness As required Elbow Assessment