Download
1 / 39
390 likes | 532 Vues
Evolving Role of the Respiratory Care Practitioner. Utilizing the expertise of the r espiratory practitioner to improve operational efficiency. The changing face of healthcare delivery.

E N D
Evolving Role of the Respiratory Care Practitioner Utilizing the expertise of the respiratory practitioner to improve operational efficiency
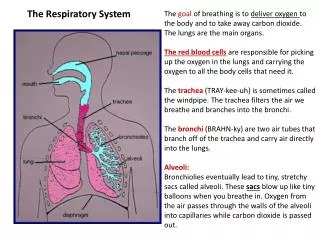
The changing face of healthcare delivery As we move from the traditional “Fee for Service” model towards an “Outcome Based Medicine” model we must consider: The health and well being of the patient As well as, The health and well being of the hospital
Evolving Role of the Respiratory Care Practitioner Goals Discuss the influence of the changing environment Review basics of the Healthcare Reform Act Gain an understanding of what impacts hospital reimbursement Discuss areas of possible improvement for patient and hospital outcomes that Respiratory Care can impact
Health Care Reform The Patient Protection and Affordable Care Act (PPACA),commonly called the Affordable Care Act (ACA) or "Obamacare", represents the most significant regulatory overhaul of the country's healthcare system since the passage of Medicare and Medicaid in 1965. Additional reforms aim to reduce costs and improve healthcare outcomes by shifting the system towards quality over quantity through increased competition, regulation, and incentives to streamline the delivery of healthcare.
Per Capita Total Current Health Care Expenditures, U.S. and Selected Countries, 2010 The U.S. is highest in per capita healthcare spending ^ 2009 data Notes: Amounts in U.S.$ Purchasing Power Parity, see www.oecd.org/std/ppp; includes only countries over $2,500. OECD defines Total Current Expenditures on Health as the sum of expenditures on personal health care, preventive and public health services, and health administration and health insurance; it excludes investment. Source: Organisation for Economic Co-operation and Development. “OECD Health Data: Health Expenditures and Financing”, OECD Health Statistics Data from internet subscription database. http://www.oecd-library.org, data accessed on 08/23/12.
5% of the population spends 50% of total healthcaredollars Concentration of Healthcare Spending in the U.S. Population, 2009 Percent of Total Health Care Spending (≥$51,951) (≥$17,402) (≥$9,570) (≥$6,343) (≥$4,586) (≥$851) (<$851) Note: Dollar amounts in parentheses are the annual expenses per person in each percentile. Population is the civilian no-ninstitutionalized population, including those without any health care spending. Health care spending is total payments from all sources (including direct payments from individuals and families, private insurance, Medicare, Medicaid, and miscellaneous other sources) to hospitals, physicians, other providers (including dental care), and pharmacies; health insurance premiums are not included. Source: Kaiser Family Foundation calculations using data from U.S. Department of Health and Human Services, Agency for Healthcare Research and Quality, Medical Expenditure Panel Survey (MEPS), Household Component, 2009.
Triple aim of healthcare policy • 3 Overlapping Problems to Solve: • Lack of access to timely and affordable healthcare for large segments of the population • Rising healthcare costs and inflation that threatens the sustainability of our legacy financing structures • Highly variable quality of care It is rare for policies to accomplish all three objectives. Most policies involve a trade-off with at least one objective.
Value Based Purchasing Value is considered a function of quality, efficiency, safety, & cost What is Hospital Value-Based Purchasing? The Hospital Value-Based Purchasing (VBP) Program is a Centers for Medicare & Medicaid Services (CMS) initiative that rewards acute-care hospitals with incentive payments for the quality of care they provide to people with Medicare. Process of Care Measures Hospital Acquired Conditions Patient Experience
Value Based Purchasing Incentive Payments will be based on Clinical Outcomes – 70% Patient Satisfaction – 30%
Value Based Purchasing • Readmissions • All-cause; AMI, HF, and Pneumonia • Process of Care Measures • 13 clinical process-of-care measures; AMI, HF, Pneumonia, Surgical Care Improvement, and mortality • Hospital Acquired Conditions • 12 clinical conditions that arose during their hospital stay: Air Embolism, Blood Incompatibility, Catheter Infections, DVT post orthopedic surgery, falls w/trauma, foreign bodies a/surgery, poor glycemic control, Pressure Ulcers, SSI, • Patient Experience • 8 patient experience measures; Communication w/Nurses-Doctors-Medicines, responsiveness of hospital staff, pain management, cleanliness and quietness of the hospital, discharge information, overall rating of hospital
Value Based Purchasing – Readmission Rates Current Data 30 day readmission rates for specific conditions Heart Failure 26.9% Pneumonia 20.1% COPD 22.6%
Evolving Role of the Respiratory Care Practitioner High Impact Categories Length-of-Stay Case Mix Index Relationship with all health care providers/facilities Optimizing proven evidence based practices
Length of Stay Why does this matter? • Reduction in utilization • Reduced costs • Reduced complications • Increased patient satisfaction
Hospital Costs Average Costs per hospital stay $14,427* Per hospital day $3,612* per ICU stay (non-ventilated) $12,931** Average LOS in ICU (non-ventilated) 8.5 days** 1 day increase in LOS in ICU $2,401*** 1 day increase in LOS on Med/Surg $1,122*** *data from 2010 International Federation of Health Plans, ** CCM 2005 Dasta JF, et al., *** Candrilli & Mauskopf RTI health Solutions “How Much Does a Hospital Day Cost?”
Evolving Role of the Respiratory Care Practitioner Proactive, outcome based care is centered on Restoring the Natural Balance in the patient The goal of proactive-outcome based care is to; Improve patient outcomes-prevent escalation of care decrease Length of Stay minimize opportunity for bounce-back admissions (hospital or ICU)
Identify – Anticipate -Personalize Be Proactive Not Reactive Improved Outcomes with: Identification of the at-risk and chronic patient Use a multi-disciplinary team approach to determine short and long term goals for the patients health. Work with discharge planners early on. Communicate in real time Identify at risk – anticipate respiratory needs – personalize the care plan
Length of Stay Case Study Company Type: Not-for-Profit Medical Center Project Title: Respiratory Length of Stay (LOS) Reduction Tools Used: Juran Lean Six Sigma – Rapid Improvement Event and DMAIC Project Timeline: Six months Total Savings: Reduced specified Respiratory Diagnoses Related Group’s (DRGs) LOS by 1.4 days, from 7.7 to 6.3 days. Savings of $495,600 over the six months following implementation. When all patients affected are considered, the total six month savings rises to $636,900. Juran Institute, Inc.
Case Study How did they achieve this improvement? • Voice of the Customer • Ability to respond to patient/family needs • Safe, high quality care is consistently provided • Atmosphere of partnership and trust between hospital, PCP, and ancillary staff • Timely, clear planning of patient care • Test orders and results that are obtained quickly, easily, and accurately
Case Study How did they achieve this improvement? • Value-Add and Non-Value Add • Unit secretaries ordering wrong tests • Transportation delays • Labs and test results not ready when MD makes rounds • Decline in function due to failure of timely assessments and interaction; ambulation, increased 02 demand, WOB increase, etc.
Case Study How did they achieve this improvement? • Measurable Improvements • Real-time results log-alerts staff when labs are due • New PT screening process that involves case management and ancillary staff • Added/revamped Ventilation Weaning protocol • Developed a palliative care program • Daily huddle to identify appropriate patient care level, anticipate discharge date, medical management plan, and barriers to patient progress.
Length of Stay “Inpatient” vs. “Outpatient/Observation” Specific criteria (based on severity of illness and intensity of service) must be met in order to admit a patient to the hospital. A patent can be receiving any service anywhere in the hospital (Radiology, Emergency Department, or nursing floor) and still be considered an “outpatient” according to CMS guidelines. Medicare Part B covers outpatient hospital and physician services. Generally, this means you pay a copayment for each individual outpatient hospital service. Medicare requires a “qualifying hospital stay” in order for Medicare A to cover care within a skilled nursing facility. Healthcare Reform Magazine; published July 06, 2011
Length of Stay “Inpatient” vs. “Outpatient/Observation” • Hospital reimbursement difference • Outpatient is approximately 28% of a MSDRG payment • Average observation payment $1,600 • Average MSDRG payment $5,600 • Patients subject to co-pay • Typical 20% • Many non-covered drugs considered self delivery • MDI charge can range from $200 - $700 • Nebulized medication $7.00 • Patients must submit to Medicare Part D for reimbursement
Case Mix Index Case mix index (CMI) is a relative value assigned to a diagnosis-related group (DRG) of patients in a medical care environment. The CMI value is used in determining the allocation of resources to care for and/or treat the patients in the group. Drives the GMLOS of the patient (expected mean length of stay) The CMI value of a hospital can be used to adjust the average cost per patient (or per day) for a given hospital. Is the multiplier for reimbursement from the hospitals Base Rate.
Inpatient Prospective Payment System (IPPS) • Each Medicare patient (discharge) is classified into a DRG • Principal Diagnosis (why the patient was admitted) • Major Complications and Comorbidities or Complication/Comorbidity (MCC/CCs) • Surgical Procedures • Age (e.g., Newborn) • Gender • Discharge Disposition (routine, transferred or expired)
DRGs and Severity • DRGs and CMI can be used to evaluate quality of care that is expected to be received: • Clinically similar groups • Analysis of treatment protocols • Related condition or demographic distribution • DRGs and CMI reflect utilization of services (DRGs include the average # of resources needed to treat each clinical group) • DRGs determine the calculation for Relative Weight (RW) or resources consumed…
DRG Relative Weight Definition Relative Weight (RW): = An assigned weight (number/figure) to reflect the resource consumption associated with each DRG. The higher the RW the higher the resources used to treat that diagnostic grouping thus the higher PPS payment to the hospital. The greater the # of resources needed to treat a given patient and the greater the intensity of these services within that DRG. DRG RW X Base Rate (hospital specific) = Hospital Payment ($).
Case-Mix Index - BRMC Medicare target 1.630 All-payor target 1.540 30
Pneumonia DRG 195 Simple PNA & Pleurisy w/o CC/MCC Relative Weight 0.6997 GMLOS 2.9 DRG 194 Simple PNA & Pleurisy w CC Example of CC is CHRONIC RESPIRATORY FAILURE Relative Weight 0.9771 GMOLS 3.8 DRG 193 Simple PNA & Pleurisy w MCC Example of MCC is ENCEPHALOPATHY Relative Weight 1.4550 GMLOS 5.0
COPD DRG 192 COPD w/o CC/MCC Relative Weight 0.7120 GMLOS 2.8 DRG 191 COPD w CC Example of CC is HYPONATREMIA Relative Weight 0.9343 GMLOS 3.5 DRG 190 COPD w MCC Example of MCC is SEVERE PROTEIN CALORIE MALNUTRITION Relative Weight 1.1708 GMLOS 4.2
Sepsis DRG 872 Septicemia or Severe Sepsis w/o 96+ Hrs w/o MCC Relative Weight 1.0687 GMLOS 4.1 DRG871 Septicemia or Severe Sepsis w/o 96+ Hrs w MCC Example of MCC is PNEUMONIA Relative Weight 1.8527 GMLOS 5.1
Evolving Role of the Respiratory Care Practitioner Improved Relationships with all health care providers/facilities Adversary to Collaborative Long Term Acute Care Rehabilitation Hospitals Skilled Nursing Facilities Home Health
PAC Utilization Rates Nationwide, about four out of every ten Medicare patients are discharged from acute hospitals to a post-acute care setting (SNF, Home Health, LTAC or Rehab Hospital)
Readmission Concerns High percentage of discharges to post acute care are readmitted within 30 days. CHF, AMI, and Pneumonia readmission rates by SNF providers can have wide variability 15% to 60%. (VBP) Most readmissions from PAC providers come through the ED Significant opportunity exists to enhance communication, education and information-sharing processes at hand-off to improve continuity of care and mitigate the risk of avoidable transfers back to the hospital.
Improved Relationships with all Health Care Providers/Facilities • Understand your local payor mix and what is considered in network • Understand admitting criteria • Educate YOUR staff on patient population • Develop working relationships with your peer • This may not be a Respiratory Therapist • Understand the strengths and weakness of the facility
Improved Relationships with all Health Care Providers/Facilitiesa Some facilities may not have Respiratory Therapist on staff or limited hours Evaluate the equipment and intensity of care Discuss the personalized care plan with the PAC team Offer assistance; training, vendor connections, equipment evaluation Basic protocol development Point of contact for questions
Operationalizing Proven Evidence Based Practices What are the next steps for Respiratory Care?
What are the next steps for Respiratory Care? • Self evaluation of the daily role • What we doing • Awareness of Hospital metrics • LOS, CMI, HAC, Readmission rates, Service Scores • Relationships • Administration, medical staff, PAC providers • Clinical practice • protocols • Process Improvement • Knowledge of proven tactics; lean methodology, Six Sigma, etc.