Download
1 / 64
690 likes | 1.25k Vues
Feeding Patients: Oral Diets and Enteral and Parenteral Nutrition Chapter 15. Feeding Patients: Hospital Food and Enteral and Parenteral Nutrition. Up to 40% of hospitalized patients are malnourished Hospital food may be refused because: It is unfamiliar Tasteless (e.g., cooked without salt)

E N D
Feeding Patients: Oral Diets and Enteral and Parenteral NutritionChapter 15
Feeding Patients: Hospital Food and Enteral and Parenteral Nutrition • Up to 40% of hospitalized patients are malnourished • Hospital food may be refused because: • It is unfamiliar • Tasteless (e.g., cooked without salt) • Inappropriate in texture (e.g., pureed meat) • Religiously or culturally unacceptable • Served at times when the patient is unaccustomed to eating
Feeding Patients: Hospital Food and Enteral and Parenteral Nutrition (cont’d) • Meals may be withheld or missed • Inadequate liquid diets may not be advanced in a timely manner • Giving the right food to the patient is one thing; getting the patient to eat (most of it) is another
Oral Diets • Easiest and most preferred method of providing nutrition • Oral diets may be categorized as: • “Regular” • Modified consistency • Therapeutic
Oral Diets (cont’d) • Normal, regular, and house diets • Regular diets are used to achieve or maintain optimal nutritional status • Regular diets are adjusted to meet age-specific needs throughout the life cycle • Diet as tolerated (DAT)
Oral Diets (cont’d) • Modified consistency diets • Modified-consistency diets include: • Clear liquid • Mechanically altered diets
Oral Diets (cont’d) • Modified consistency diets • Clear liquid diets may be used: • After surgery • In preparation for bowel surgery or procedures • When oral intake resumes after a prolonged period • Most patients can tolerate a regular diet for their second postoperative meal
Oral Diets (cont’d) • Modified-consistency diets (cont’d) • Mechanically altered diets contain foods that are chopped, ground, pureed, or soft • Diets prepared in a blender provide food in liquid form • Dysphagia diets are another variation of modified-consistency diets
Oral Diets (cont’d) • Therapeutic diets • Therapeutic diets differ from a regular diet • Used for the purpose of preventing or treating disease or illness • Nutritional supplements • Some patients are unable or unwilling to eat enough food to meet their requirements
Oral Diets (cont’d) • Nutritional supplements (cont’d) • Categories of supplements include: • Clear liquid supplements • Milk-based drinks • Prepared liquid supplements • Specially prepared foods
Oral Diets (cont’d) • Nutritional supplements (cont’d) • Liquid supplements are: • Easy to consume • Are generally well accepted • Tend to leave the stomach quickly • A good choice for between-meal snacks
Question • What type of diet is a dysphagia diet? a. Prepared in a blender b. Liquid c. Modified consistency d. Mechanically ground
Answer c.Modified consistency Rationale: Dysphagia diets are another variation of modified-consistency diets.
Oral Diets (cont’d) • Liquid supplements • Allow the patient to taste test several options available • Explain the rationale for adding supplements and closely monitor acceptance • Given on a rotation schedule
Oral Diets (cont’d) • Modular products • Less frequently used option for maximizing a patient’s oral intake • Generally composed of a single nutrient • Disadvantages: • Quality control (calculation errors) • Bacterial contamination • Higher costs than standard formulas
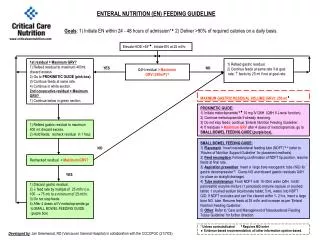
Enteral Nutrition • A way of providing nutrition for patients who are unable to consume an adequate oral intake but have at least a partially functional GI tract that is accessible and safe to use • Enteral nutrition (EN) may augment an oral diet or may be the sole source of nutrition
Candidates for Tube Feeding • Patients who: • Have problems chewing and swallowing • Have prolonged lack of appetite • Have an obstruction, fistula, or altered motility in the upper gastrointestinal tract • Are in a coma • Have very high nutrient requirements
Enteral Nutrition (cont’d) • Contraindicated when the gastrointestinal tract is nonfunctional • Patients who receive enteral nutrition experience less septic morbidity and fewer infections and complications than patients who receive parenteral nutrition • Significantly less costly than parenteral nutrition • Has not been proven to reduce the length of the hospital stay and improve mortality
Enteral Nutrition (cont’d) • More high-quality trials are needed • Factors that influence how and what is used to feed patients enterally include: • The patient’s calorie and protein requirements • Ability to digest nutrients • Feeding route
Enteral Nutrition (cont’d) • Factors that influence how and what is used to feed patients enterallyinclude (cont’d): • Characteristics of the formula • Equipment available • Method of delivery
Question • Enteral nutrition is a way of providing nutrition for people who have an inadequate oral intake. What is the other criteria for enteral nutrition? a. Partially functioning GI tract b. Nonfunctioning GI tract c. Obstructed GI tract d. Patient is comatose
Answer • Partially functioning GI tract Rationale: Enteral nutrition (EN) is a way of providing nutrition for patients who are unable to consume an adequate oral intake but have at least a partially functional GI tract that is accessible and safe to use.
Enteral Nutrition (cont’d) • Feeding route • Depends on the patient’s medical status and the anticipated length of time the tube feeding will be used • Transnasal tubes • Nasogastric (NG) tube is the most common • Generally used for tube feedings of relatively short duration
Enteral Nutrition (cont’d) • Feeding route (cont’d) • Ostomy feedings are preferred for permanent or long-term feedings • Percutaneous endoscopic gastrostomy (PEG) tubes are placed with the aid of an endoscope
Enteral Nutrition (cont’d • Formula characteristics • Formulary of various enteral products available within major categories • Are designed to provide complete nutrition
Enteral Nutrition (cont’d) • Protein • Enteral formulas are classified by the type of protein they contain • Standard formulas • Made from whole proteins or protein isolates • Provide 34 to 43 g protein/liter
Enteral Nutrition (cont’d) • Protein (cont’d) • Variations • High in protein • High in calories • Fiber enriched • Disease-specific formulas designed for patients with diabetes, immune system dysfunction, renal failure, or respiratory insufficiency
Enteral Nutrition (cont’d) • Protein (cont’d) • Hydrolyzed protein formulas • Completely hydrolyzed formulas contain only free amino acids as their source of protein • Partially hydrolyzed formulas contain proteins that are broken down
Enteral Nutrition (cont’d) • Protein (cont’d) • Hydrolyzed protein formulas • Intended for patients with impaired digestion or absorption • Disease-specific formulas are available for liver failure, HIV/AIDS, and immune system support
Enteral Nutrition (cont’d) • Calorie and nutrient density • Calorie density of a product determines the volume of formula needed • Routine formulas provide 1.0 to 1.2 cal/mL • High-calorie formulas provide 1.5 to 2.0 cal/mL • Nutrient density • Varies among formulas • Ranges from 1,000 to 2,000 mL/day
Enteral Nutrition (cont’d) • Water content • Varies with the caloric concentration • Formulas that provide 1.0 cal/mL provide 850 mL of water/liter • High calorie formulas is lower at 690 to 720 mL/L • Adults generally need 30 to 40 mL/kg/day • Need additional free water
Enteral Nutrition (cont’d) • Other nutrients • High-fat formulas are available for patients with respiratory disease • Modified-fat formulas are designed for patients with malabsorption • Diabetic formulas are available • Electrolyte-modified formulas for renal disease
Enteral Nutrition (cont’d) • Fiber and residue content • Terms fiber and residue are frequently used interchangeably • Fiber • Stimulates peristalsis, increases stool bulk, and is degraded by gastro-intestinal bacteria • Combines with undigested food, intestinal secretions, and other cells to make residue
Enteral Nutrition (cont’d) • Fiber and residue content • Residue content of enteral formulas varies greatly • Hydrolyzed formulas are essentially residue free • Most standard formulas are low in residue • Formulas prepared in a blender are a natural source of fiber
Enteral Nutrition (cont’d) • Osmolality • Determined by the concentration of sugars, amino acids, and electrolytes • Isotonic formulas have approximately the same osmolality as blood • Some patients develop diarrhea when a hypertonic formula is infused
Question • Is the following statement true or false? Routine formulas provide 1.5 to 2 cal/mL.
Answer False. Rationale: The calorie density of a product determines the volume of formula needed to meet the patient’s estimated needs. Routine formulas provide 1.0 to 1.2 cal/mL, whereas high-calorie formulas provide 1.5 to 2.0 cal/mL.
Enteral Nutrition (cont’d) • Equipment • Tubing size and pump availability impact formula selection • High-fiber formulas have a high viscosity and require a large bore tube (8F or greater) to prevent clogging • Hydrolyzed formulas have very low viscosity
Enteral Nutrition (cont’d) • Delivery methods • Formulas may be given intermittently or continuously over a period of 8 to 24 hours • Type of delivery method to be used depends on the type and location of the feeding tube, the type of formula being administered, and the patient’s tolerance
Enteral Nutrition (cont’d) • Intermittent feedings • Administered throughout the day • Generally used for noncritical patients, home-tube feedings, and patients in rehabilitation • More closely resemble a normal intake • Allow the client freedom between feedings
Enteral Nutrition (cont’d) • Intermittent feedings (cont’d) • Gastric residuals are checked before each feeding • Residual volumes of 200 mL or more on 2 successive assessments suggest poor tolerance • Bolus feedings • Variation of intermittent feedings • Large volume of formula delivered relatively quickly • Often cause dumping syndrome
Enteral Nutrition (cont’d) • Continuous drip method • Given at a constant rate over a 16- to 24-hour period • Recommended for feeding of critically ill clients • Continuous feedings should be interrupted every 4 hours • Cyclic feedings • Variation of continuous-drip feedings • Cyclic feedings are usually well tolerated
Enteral Nutrition (cont’d) • Initiating and advancing the feeding • Before initiating a feeding, tube placement is verified ideally by radiography, and bowel sounds are confirmed to be present • Regardless of the access route, tube feeding formulas are initiated at full strength • Initial feedings may begin at 25 to 50 mL/hour and advance by 10 to 25 mL/hour every 8 to 12 hours as tolerated until the desired rate is achieved
Enteral Nutrition (cont’d) • Initiating and advancing the feeding (cont’d) • Commonly recommended maximum flow rate for gastric feedings is 125 mL/hr • Using a standard feeding progression schedule helps to ensure timely progression of feedings to the goal rate • Tolerance may be a problem for patients who are malnourished, who are under severe stress, or who have not eaten in a long time
Enteral Nutrition (cont’d) • Tube feeding complications • GI, metabolic, and respiratory complications are possible • Aspiration is the most serious potential complication • More common than large-volume aspirations is a series of clinically silent small aspirations • Increases the risk of aspiration-related pneumonia
Enteral Nutrition (cont’d) • Giving medications by tube • Should never be given while a feeding is being infused • Some drugs become ineffective if added directly to the enteral formula • Ensure the tube is flushed with 15 to 30 mL of water before and after the drug is given
Enteral Nutrition (cont’d) • Transition to an oral diet • Goal of diet intervention is to ensure an adequate nutritional intake while promoting an oral diet • Gradually increase meal frequency until 6 small oral feedings are accepted
Question • What is the commonly recommended maximum flow rate for gastric feedings? a. 75 mL/hr b. 100 mL/hr c. 125 mL/hr d. 150 mL/hr
Answer c. 125 mL/hr Rationale: The commonly recommended maximum flow rate for gastric feedings is 125 mL/hr; higher volumes may increase the risk of aspiration.
Parenteral Nutrition • Developed in the 1960s • Infusion of a nutritionally complete, hypertonic formula • Life-saving therapy in patients who have a nonfunctional GI tract • Also used for other clinical conditions such as critical illness, acute pancreatitis, liver transplantation, AIDS, and in patients with cancer receiving bone marrow transplants