Download
1 / 25
260 likes | 387 Vues
The role of specialist pharmacist in nutrition support. Emma Canavan Lead Pharmacist Nutrition. Overview. What is my role Nutrition Parenteral nutrition Patient assessment Components of PN Feeding Tubes Workshop feeding tubes. How I got into nutrition.

E N D
The role of specialist pharmacist in nutrition support Emma Canavan Lead Pharmacist Nutrition
Overview • What is my role • Nutrition • Parenteral nutrition • Patient assessment • Components of PN • Feeding Tubes • Workshop feeding tubes
How I got into nutrition • Graduated 2008 Liverpool John Moores University • Qualified August 2009 • 2010 Manchester Children’s Hospital • 2012 Birmingham Children’s Hospital • 2014 lead for nutrition at Heart of England Hospitals
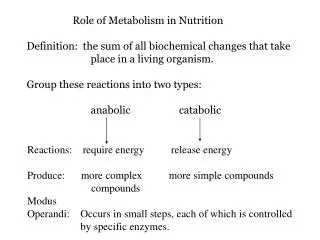
Nutrition team • NICE and BAPEN recommend that all hospitals have a nutrition team made up of a Consultant(s), specialist nutrition nurse(s), dietician(s) and pharmacist(s). These specialists provide training, advice, guidance and recommendations for all types of nutrition within the hospital
My Role • Lead pharmacist Women’s and Children’s services and nutrition • Active member and occasional lead of parenteral nutrition MDT ward round and clinic • Advise on feeding tubes and unlicensed medicines • Occasional advise on enteral feeds
Nutrition Team • Many types of nutrition service • Parenteral Nutrition • Enteral Nutrition only • Paediatric/neonatal • As a pharmacist you can have an active role in all of these
Parenteral Nutrition (PN) is the administration of nutrition via the intravenous route.
NICE guidance CG32 • Nutrition Support in Adults • Malnourished patients • Inadequate or unsafe oral and/or enteral intake • A non-functional, inaccessible or perforated gastrointestinal tract
Malnutrition • NICE definition of malnutrition, patients with • A BMI of <18.5kg/m2 • Unintentional weight loss of greater than 10% within the last 3-6 months • Or a BMI of <20kg/m2 with an unintentional weight loss greater than 5% in the last 3-6 months
Indications for PN in adults • Prolonged ileus. • Gastrointestinal fistula. • Anastomotic leak • Post operative states where oral or enteral feeding is contraindicated for more than 4-5 days e.g. multiple injuries(Campos 1992) • Malabsorption or where bowel rest is required, e.g. short bowel syndrome, severe inflammatory bowel disease, severe pancreatitis • Severe mucositis • Severe radiation enteritis • Graft versus Host disease • Chylous leaks
Contraindications to PN • A functioning and accessible GI tract • Treatment for less than 5 days in patients who are not malnourished • When the risks of PN outweigh the benefits • Sepsis • Raised INR (>1.4) • No vascular access
Starting PN • Caloric Requirements • 25-35Kcals/kg – 0.14g/kg of nitrogen • Fluid requirements • 25-30ml/kg • Electrolytes • Sodium – 1mmol/kg • Potassium – 1mmol/kg • Phosphate – 0.3-0.5mmol/kg (20mmol/day) • Magnesium – 0-15mmol/day (10mmol) • Vitamins and trace elements
PN components • Macronutrients • Lipid - Usually made from soya or fish oils • 25g lipid = 225Kcal • Carbohydrates - High calorie energy source • 25g glucose = 100Kcal • Protein - written as grams of nitrogen: 0.16g/N = 1g amino acid • Daily requirements ~0.14g N/kg/day • Fluid • Micronutrients • Vitamins • Trace elements
Routes Of Enteral Tube Feeding Feeding into the Stomach or into the Small Bowel. Main routes of enteral tube feeding used include: Intranasal insertion: • Nasogastric(NG) • Usually inserted on the ward or in radiology • Aspirate pH of 5.5 or below • Used to feed into the stomach • Nasojejunal(NJ) • Usually inserted in Endoscopy (or in ITU) • Aspirate pH of 7.0 or above • Used to feed into the Jejunum (Small bowel) Percutaneous/Surgical insertion: • Percutaneous Endoscopic Gastrostomy (PEG) • Usually inserted in Endoscopy or Theatre • Used to feed into the Stomach • Variations include PEGJ and PEJ • Radiologically Inserted Gastrostomy (RIG) • Inserted in Radiology • Used to feed into the stomach • Surgical Jejunostomy (Surg-Jej) • Inserted in Theatre • Used to feed into the stomach
Unlicensed/off-label In the UK it is unlawful for any person to sell or supply a medicine without an appropriate marketing authorisation. Doctors, dentist and veterinarians are the only people exempt from this Act. They can advise that a drug be used in an unlicensed/off license way. You take liability away from the manufacturer when medications are administered outside of the license See Drug Safety Update, April 2009.
Considerations The patient Does the patient need medications via the feeding tube or can they take them orally? Where is the tube placed? Reduced absorption pH Delivery beyond usual site of absorption Reduced transit time
Considerations cont’d… Tube size, length and type Types of feed and how they are being fed The drugs Are there liquid formulations available? Do the medications have a narrow therapeutic window? Legality
Interactions Interaction with feeds Physiological Physical Chemical Drugs can also affect the taste of food and the appetite of the patient Physical interaction with feeding tube Carbemazepine has been shown to interact with PVC feeding tubes causing reduced delivery of drugs
Drug Related Factors to Consider Is the drug needed? Is an alternative route available? Transdermal, buccal, sublingual Is there a suitable dosage form available? Does it come as a suspension, syrup, liquid. Ensure that the formulation is not modified/ slow release Where is the drug absorbed? Some drugs may be require the pH of the gastric juices to be absorbed Tubes placed in the jejunum may decrease the time drugs are in contact with GI tract, reducing absorption. Does it interact with feeds or tubes?
Preventing Blockages Effective flushing after enteral feeds stopped. Effective flushing before each drug is given Give drugs individually – do not mix If crushing tablets ensure adequately crushed and suspended Care with the use of suspensions, mups and dispersible tablets down small bore tubes e.g. omeprazole mups Feed is the most common cause of tube blockage
Unblocking Tubes Prevention is better than cure Adequate flushing before and after doses. Care in fluid restricted patients – may require air flushing Use of mechanical devices for unblocking Pancreatic enzymes Must be prescribed. Do not use acidic solutions to unblock e.g. coca cola