Download
1 / 49
580 likes | 1.08k Vues
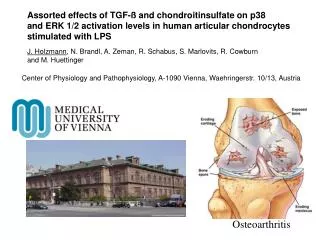
Osteoarthritis and exercise. Sirintorn Chansirikarnjana MD.Msc.(Geriatric Med) Chief, Division of Geriatric Medicine Department of Medicine Ramathibodi Hospital. Osteoarthritis. Age > 50 years Hereditary for hand osteoarthritis

E N D
Osteoarthritis and exercise Sirintorn Chansirikarnjana MD.Msc.(Geriatric Med) Chief, Division of Geriatric Medicine Department of Medicine Ramathibodi Hospital Sucheera
Osteoarthritis • Age > 50 years • Hereditary for hand osteoarthritis • Insidious onset of joint pain, progress slowly over months to years • Mono/oligo arthralgia (knee, hip) > polyarthalgia (fingers) • No or only mild inflammation • Develops symptom when standing or prolong using • Improves with rest, may have gelling phenomenon • Can be associated with crystal-induce synovitis Sucheera
Symptoms and signs • Joint involvement : common- DIP, PIP, first CMC, hip, knee, lumbar and cervical spine rare- MCP, MTP, wrist, elbow • Systemic symptom : rare • Localized symptoms : tenderness, crepitus and cracking • Sign : mild joint enlargement with firm consistency • Joint effusion : little or none Sucheera
JOINT LOCATION Weight-bearing joints • femoral head and knee joints decreased progressively with age, but not in the talus • knee joint chondrocytes exhibit more interleukin (IL)-1 receptors than ankle joint chondrocytes • knee chondrocytes express mRNA for matrix metalloproteinase (MMP)-8 Sucheera
Laboratory • ESR: usually normal • CBC : normal • RF, ANA : negative • Synovial fluid analysis : good viscosity with normal mucin clot; modest increase in leukocyte number, presence of fibrils an debris(wear particles) R/o septic joint or crystal Sucheera
Radiographicfindings • Narrowing of joint space • Subchondral bony sclerosis(eburnation) • Marginal osteophyte formation • Bone cysts and bony collapse • Gross deformity with subluxation and loose bodies • Articular cartilage ulceration • New bone formation • Proliferation of cartilage and bone • Subchondral microfractures • Ligamentous laxity as a result of mechanical forces Sucheera
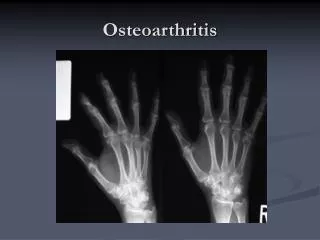
Knee Osteoarthritis • Non uniform loss of joint space • No erosion • No demineralization • Subchondral sclerosis • Osteophyte formation Sucheera
Hand Osteoarthritis Bouchard’s node Heberden’s node Sucheera
Erosive osteoarthritis • Hereditary, postmenopausal woman • Clinical resemble RA • PIP, DIP, CMC jt. • Painful inflammatory episode • Jointdeformity, ankylosis • Film: joint space narrowing, spur formation , subchondral bone sclerosis, prominent bony erosion • Lab: RF, ANA - neg Sucheera
Current Treatment of Osteoarthritis • Non-Pharmacologic Therapy • Patient education • Programmed exercises • Weight loss • Joint protection • Thermal modalities • Surgical Approaches • Arthroscopic debridement • Osteotomy • Total joint arthroplasty • Pharmacologic Therapy • Nonopioid analgesics (e.g., acetaminophen) • Topical analgesics (e.g., capsaicin) • Nonsteroidal anti-inflammatory drugs • Intra-articular steroid • Intra-articular hyaluronate • Opioid analgesics Sucheera
NSAID gastropathy • NSAID-related GI toxicity is most common serious drug-induced toxicity1 • Dyspepsia occurs in about 15% of patients2 • Prevalence of upper GI ulcers is 15–311 • Higher risk of developing gastric than duodenal ulcers3,4 • Risk of complications increases 4-fold4 • Relative risk of bleeding 3.091 • Relative risk of perforation 5.931 • Relative risk of death 7.621 1. Sung et al., J Gastroenterol Hepatol 2000; 15: G58–68. 2. Larkai et al., J Clin Gastroenterol 1989; 11: 158–62. 3. Graham et al., Ann Intern Med 1993; 119: 257–62. 4. Hawkey, Gastroenterol 2000; 119: 521–35. Sucheera
Risk Factors for Ulcer Complications • Definite • Advanced age (substantial risk after age 65) • Prior ulcer disease or ulcer complications • High-dose, multiple NSAIDs (including low-dose aspirin) • Concomitant use of anticoagulants • Concomitant use of corticosteroid therapy • Serious systemic disorder • Possible • Cigarette smoking • Alcohol consumption • Infection with Helicobacter pylori Singh et al., J Rheumatol 1999; 26(Suppl 56): 18-24. Larkai et al., J Clin Gastroenterol 1989; 11: 158–62. Graham et al., Ann Intern Med 1993; 119: 257–62. Hawkey, Gastroenterol 2000; 119: 521–35. Sucheera
Risk factors for serious GI complications • Age and history of ulcer are strong predictors of ulcer complications • Risk of hospitalisation or death1: • 3/1000 patient-years for patients under 63 years • 19/1000 patient-years for patients aged 63–75 years • 42/1000 patient-years for patients over 75 years • Relative risk of ulcer complications1: • 2.9 for a history of dyspepsia • 6.1 for a history of uncomplicated ulcers • 13.5 for a history of bleeding ulcers • Men have a 2-fold higher risk of developing complications than women2 1. Sung et al., J Gastroenterol Hepatol 2000; 15: G58–68. 2. Hernández-Díaz & García Rodríguez, Arch Intern Med 2000; 160: 2093–99. Sucheera
Complications associated with NSAID dose and duration • The risk of ulcer complications increases with NSAID daily dose1: • Low dose: relative risk 3.0 (95% CI, 2.6–3.4) • Medium dose: relative risk 4.1 (95% CI, 3.6–4.5) • High dose: relative risk 6.9 (95% CI, 5.8–8.1) • NSAIDs increase the risk of ulcer complications in new and long-term users alike: • 1–30 days’ NSAIDs: relative risk 5.7 (95% CI, 4.9–6.6) • 181–365 days’ NSAIDs: relative risk 5.1 (95% CI, 3.9–6.5) • Relative risk drops when NSAIDs are stopped and returns to baseline within about 2 months Hernández-Díaz & García Rodríguez, Arch Intern Med 2000; 160: 2093–99. Sucheera
Rx of NSAID-induced PU disease • Discontinue use of NSAIDs or substitute with less toxic agents • Low-toxicity NSAIDs or COX-2 inhibitors • Suppress acid secretion • Normal-dose PPI therapy • High-dose H2RA therapy • Use mucosal protectants • Misoprostol (side-effects can be problematic) Seager & Hawkey, BMJ 2001; 323: 1236–9. Silverstein et al., Ann Intern Med 1995; 123: 241–9. Graham et al., Ann Intern Med 1993; 119: 257–62. Yeomans et al., N Engl J Med 1998; 338: 719–26. Sucheera
Acid suppression in NSAID-induced PU • Antacids • Limited efficacy, especially in preventing gastric ulcer • H2RAs • Effective in preventing gastric ulcer; some drug interactions, well tolerated • PPIs • More effective than H2RAs for healing NSAID-induced ulcers, well tolerated Seager & Hawkey, BMJ 2001; 323: 1236–9. Goldstein et al., Gut 1999; 25(Suppl V): A101. Yeomans et al., N Engl J Med 1998; 338: 719–26. Sucheera
NSAIDs and Cardiovascular • All NSAIDs : • Salt and water retention • Increase BP • May cause CHF in patient with cardiac problem • Interfere with antihypertensive drugs • ACEI • Beta blocker • Calcium antagonist Sucheera
Effects and CV Risk COX-2 COX-1 Sucheera
COX-2 selective inhibitors VS NSAID: balancing GI and CV risk Conclusion: Calculating annualized event rates for GI and CV harm shows that while complicated GI events occur more frequently with NSAIDs than coxibs, serious CV events occur at approximately equal rates. For each coxib, the reduction in complicated upper GI events was numerically greater than any increase in APTC events. R A Moore, et.al : BMC Musculoskeletal Disorders 2007, 8:73 Event rate difference (coxib-NSAID) per 1000 per year Sucheera
Shared Toxicities of NSAIDs Renal • Sodium retention • Weight gain and edema • Hypertension • Type IV renal tubular acidosis and hyperkalemia • Acute renal failure • Papillary necrosis • Acute interstitial nephritis • Accelerated chronic renal failure Sucheera
Indication for COX-2 Inhibitors • Age> 70 yr. with nocardiovascular, renal or hepatic diseases • History of aspirin induced asthma • History of majorpeptic ulcer complication (bleeding, obstruction, perforation) • Continue GI complication even after adding gastroprotective agents to conventionalNSAIDs • Pre and post operative pain (short course) Sucheera
Exercise Prescriptionfor Special Populations Advanced age • Resistance training is recommended by most health promotion organizations for its effects on maintenance of strength, muscle mass, bone mineral density, functional capacity, and prevention and/or rehabilitation of musculoskeletal problems (eg,low back pain) Emedicine.medscape Jun 24, 2009 Amer Suleman, MD; Kyle D Heffner, MS, CPFT, CCT Sucheera
Exercise Prescriptionfor Special Populations Advanced age • In elderly individuals, resistance training is both safe and beneficial in improving flexibility and quality of life Emedicine.medscape Jun 24, 2009 Amer Suleman, MD; Kyle D Heffner, MS, CPFT, CCT Sucheera
Contraindications Absolute contraindications to exercise include • Suspected acute coronary syndrome • 3rd-degree heart block • Uncontrolled hypertension • Acute heart failure • Uncontrolled diabetes mellitus Merch Manaul April 2009 by Brian D. Johnston; Paul L. Liebert, MD Sucheera
Contraindications Relative contraindications include • Cardiomyopathy • Valvular heart disease • Complex ventricular ectopy Merch Manaul April 2009 by Brian D. Johnston; Paul L. Liebert, MD Sucheera
Screening 1 Detecting cardiac disorders and Physical limitations to exercise For sedentary patients who plan to begin intense exercise, stress testing is indicated if they have any of the following: Merch Manaul April 2009 by Brian D. Johnston; Paul L. Liebert, MD Sucheera
Screening 2 • Known coronary artery disease • Symptoms of coronary artery disease • > 2 cardiac risk factors (hypercholesterolemia, hypertension, obesity, sedentary lifestyle, smoking, family history of early coronary artery disease) • Suspected lung disease • Suspected diabetes Merch Manaul April 2009 by Brian D. Johnston; Paul L. Liebert, MD Sucheera
Physical Activity and Public Health in OlderAdults: Recommendation from the AmericanCollege of Sports Medicine and theAmerican Heart Association Sucheera
30 minutes a day of aerobic activity five days a week • Resistance training exercise to reduce stress on joints, bones and soft tissues; • Add flexibility and balance to the mix Sucheera
บริหารกล้ามเนื้อ ชะลอ ข้อเสื่อม Sucheera
กล้ามเนื้อส่วนคอ Sucheera
การบริหารกล้ามเนื้อคอการบริหารกล้ามเนื้อคอ เอียงคอ ซ้าย - ขวา Sucheera
การบริหารกล้ามเนื้อคอการบริหารกล้ามเนื้อคอ หันหน้าไปไหล่ ซ้าย - ขวา Sucheera
การบริหารกล้ามเนื้อคอการบริหารกล้ามเนื้อคอ ใช้มือดันหน้าผาก-ก้มศีรษะไปด้านหน้า Sucheera
การบริหารกล้ามเนื้อคอการบริหารกล้ามเนื้อคอ ประสานมือหลังศีรษะ-ดันศีรษะไปด้านหลัง Sucheera
การบริหารกล้ามเนื้อคอการบริหารกล้ามเนื้อคอ ใช้มือดันศีรษะด้านข้าง-เอียงศีรษะไปด้านข้าง (ทำสลับ ซ้าย-ขวา) Sucheera
กล้ามเนื้อข้อเข่า Sucheera
การบริหารกล้ามเนื้อข้อเข่าการบริหารกล้ามเนื้อข้อเข่า ห้อยเท้า ผูกน้ำหนักที่ข้อเท้า ½ - 1 กิโล ทั้ง 2 ข้าง (ทำวันละ 1-3 ครั้ง ครั้งละ 5-15 นาที) Sucheera
การบริหารกล้ามเนื้อข้อเข่าการบริหารกล้ามเนื้อข้อเข่า วางเท้าบนเก้าอี้ พร้อมกดเข่าลงนาน 5-10 วินาที แล้วพัก 1 นาที (ทำวันละ 3 ครั้ง) Sucheera
การบริหารกล้ามเนื้อข้อเข่าการบริหารกล้ามเนื้อข้อเข่า เกร็งกล้ามเนื้อต้นขา-กระดกข้อเท้ายกเท้าขึ้นค้างไว้ 5-10 วินาที (ทำวันละ 3 ครั้ง) Sucheera
การบริหารกล้ามเนื้อข้อเข่าการบริหารกล้ามเนื้อข้อเข่า เกร็งกล้ามเนื้อต้นขา-กระดกข้อเท้ายกเท้าขึ้นสูงจากพื้น 1 ฟุต ค้างไว้ นับ 1-10 สลับกัน 2 ข้าง (ทำวันละ 3 ครั้ง) Sucheera
กล้ามเนื้อข้อสะโพก Sucheera
การบริหารกล้ามเนื้อข้อสะโพกการบริหารกล้ามเนื้อข้อสะโพก เกร็งกล้ามเนื้อต้นขา-กระดกข้อเท้ายกเท้าขึ้น กางขาออกด้านข้างในท่าตะแคง สลับกัน 2 ข้าง (ทำวันละ 3 ครั้ง) Sucheera
การบริหารกล้ามเนื้อข้อสะโพกการบริหารกล้ามเนื้อข้อสะโพก เกร็งกล้ามเนื้อต้นขา-กระดกข้อเท้างอเข่าขึ้น สลับกัน 2 ข้าง (ทำวันละ 3 ครั้ง) Sucheera
การบริหารกล้ามเนื้อข้อสะโพกการบริหารกล้ามเนื้อข้อสะโพก เกร็งกล้ามเนื้อต้นขา-กระดกข้อเท้ากางขาออกด้านข้าง สลับกัน 2 ข้าง (ทำวันละ 3 ครั้ง) Sucheera
การบริหารกล้ามเนื้อข้อสะโพกการบริหารกล้ามเนื้อข้อสะโพก เกร็งกล้ามเนื้อต้นขา-กระดกข้อเท้ากางขาออกด้านหลัง สลับกัน 2 ข้าง (ทำวันละ 3 ครั้ง) Sucheera