Download
1 / 27
270 likes | 754 Vues
Amputation Stump Infection. Prof Jai Kulkarni / Dr. Basu ST6 Disablement Services Centre University Hospitals of South Manchester May 2012. Is it an infected stump or not ?. Infection Continuum.

E N D
Amputation Stump Infection Prof Jai Kulkarni / Dr. Basu ST6 Disablement Services Centre University Hospitals of South Manchester May 2012
Wound Contamination: Presence of bacteria within the wound but with no host reaction. Does not delay wound healing. • Wound colonisation: Presence of bacteria in the wound which do multiply. No delay to healing and no host reaction. • Critical colonisation: Multiplication of bacteria in a wound causing a delay in healing. Increased pain with thick slough and malodour. No cellulitis.
Wound Infection Multiplication of bacteria in the wound with host reaction Erythema Pain/heat/swelling Increase in exudates Asc lymphangitis and Prox lymphadinopathy +/- Systemic symptoms
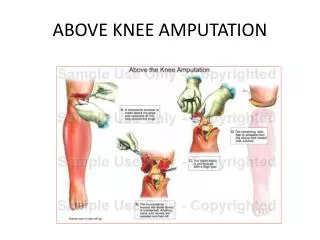
Lower limb amputations account for the majority of all amputations in the UK, with PVD and diabetes being the major reasons for surgery – 80% Within the population of patients with dysvascularity, major lower extremity amputation results in significant peri-operative morbidity and mortality. Potential wound-healing complications associated with lower limb amputation stumps include infection, tissue necrosis, pain, problems with the surrounding skin, scar adhesion, haematoma, stump oedema, osteomyelitis and dehiscence. The highest rate of surgical site infection is associated with lower limb amputations. Wound healing outcomes for amputees can be maximised by MDT working.
Wound healing complications associated with the stump of an amputee are important because in some cases these determine a patient's ability to walk with a prosthetic limb. Commonest stump-related complications were wound infection and poor healing (70%), poorly fashioned stumps (20%) and phantom pain (10%) White SA, Thompson MM, Zickerman AM, Broomhead P, Critchley P, Barrie WW, et al. Lower limb amputation and grade of surgeon. Br J Surg 1997; 84(4): 509-11. The healing rates for below- and above-knee amputations vary considerably. It is thought that a total of 90% of above-knee major amputations heal, 70% primarily, whereas for below-knee amputations, primary healing rates range between 30% and 92%, with a re-fashioning rate of up to 30%. Dormandy J, Heeck L, Vig S. Major amputations: clinical patterns and predictors. SeminVascSurg 1999; 12(2): 154-61
Wound Healing Inflammation phase with haemostasis (approx 1-7 days): Initially white blood cells are attracted to wound. Leucocytes get rid of the wound contaminants. Neutrophils assist in destroying bacteria. At 2-3 days macrophages assist in cleaning wound of bacteria Slough common at this stage. As cells engulf bacteria they float to surface of wound and die = slough Proliferation phase (approx 4-24 days): Components are a) Granulation (new wound matrix provides the scaffolding for new blood vessels). Macrophages- continue to destroy bacteria - release growth factors to attract fibroblasts - stimulate fibroblasts to produce collagen-send for endothelial cells to form new capillary loops. New capillary network formed in wound bed as well as new connective tissue b) Wound contraction: Myofibroblasts are produced. They congregate at the wound edges and contract allowing the wound edges to come together. c) Epithelialisation (resurfaces the wound): This is the re surfacing of the wound by new skin cells. New cells multiply and migrate. Process aided by moist wound environment. Wound bed must be clean and free from devitalised tissue Maturation phase (20days- 1 year): Can take up to 1 year. Re modelling of collagen into a more structured tissue occurs. Wound becomes paler and flatter as vascularisation decreases. Tensile strength improves
Unhealed stump is not always infected “Unhealed” stumps often show healing at the ends of the suture line. Unhealed over the bone. When is an unhealed stump suitable for prosthetic fitment? No standard Various centres use different regimes Small wounds ok Leave until fully healed Early walking aid only Can we apply force/friction to a dressed wound? What are the benefits of exercise? Builds muscle Helps claudication Improves general fitness
Evidence Early post-op rehabilitation results in improved functional outcomes (Friedman 1990;Munin 2001). Compression and EWAs result in quicker progression to prosthetic rehabilitation (Condie 1998). Friedmann LW. (1990) Rehabilitation of the lower extremity amputee. In: Kottke FJ, Lehmann JF, editors. Krusen’s handbook of physical medicine and rehabilitation (4th edition) Philadelphia: WB Saunders Company p 1024-69. Munin MC, Espejo-DeGuzman MC, Boninger ML, Fitzgerald SG, Penrod LE, Singh J (2001) Predictive factors for success in early prosthetic ambulation amongst lower limb amputees. Journal of Rehabilitation Research and Development 38(4): p 379-84. Condie ME, Treweek SP, Ruclkey CV (1998). Trends in lower limb management: 3 year results from a national survey. British Journal of Surgery 85 (supp1) 23. Van Ross ERE, Abbott CA, Johnson S (2009) Effects of early mobilisation on unhealed dysvasculartranstibial amputation stumps:A clinical trial Arch Phys Med Rehab 90(4):610-17.
Advantages of Transtibial Amputations Improved function Lower energy requirement for mobilisation Easier to don/doff Reduced chance of prosthetic abandonment Improved survival Lower dependency on family/state Cheaper to rehabilitate Benefits of early mobilisation protocol: Promote TT instead of TF amputation. Prevent joint contractures/muscle wasting. Psychological boost for pts. Rehab and wound healing occur simultaneously. Optimal functional outcomes.
Infection of Stump Dermatological infection: 30% of cases Allergic Contact Dermatitis ( ACD ) frequently appears as a macular, papular, erythematous rash that is often pruritic. The liner, socks, and suspension mechanism are the usual culprits for contact dermatitis. Occurs in 1/3 rd of these cases. Cysts and sweating can be signs of excessive shear forces and components that are improperly fitted; sweating can also result from the loss of surface area Tinea infections are caused by excessive moisture – Fungal culture and treatment Skin maceration Folliculitis is an infection of the hair follicles caused by poor hygiene, sweating, and poor socket fit; treatment includes use of antiseptic cleaner and topical ointments; socket modification may be required to avoid high-pressure areas An epidermoid cyst (hydradinitis Suppurativa) is a sebaceous gland that is plugged with keratin; treatment includes the use of topical or oral antibiotics, as well as incision and drainage or excision
Is it an infected Stump Verrucose hyperplasia that has developed after choke syndrome. Choke syndrome develops when tight proximal socket impairs venous return and lack of total contact occurs between the residual limb and the prosthetic socket. Acutely, significant edema leads to weeping and blistering skin. As the choke becomes chronic, the tissues become thickened and indurated. Hemosiderin deposition causes hyperpigmentation of the skin
Infection of Stump Soft Tissue and Bony Infection Bursitis FB like - Bone wax Infected thrombosed Vascular graft Management of infection of major amputation stumps after failed femorodistal grafts. Rubin JR, Yao JS, Thompson RG, Bergan JJ; Surgery 1985; Oct . Delayed stump healing was noted to occur more commonly in the group who had undergone previous bypasses as opposed to those who had undergone primary amputation (34.8% versus 14.3%). Fourteen graft infections developed in 89 patients after amputation (15.7%), which is significantly higher than the overall 1.4% incidence of lower-extremity bypass infections that occurred during the same interval in patients with intact extremities. In addition, it was found that when infected grafts in amputated limbs were completely removed, stump healing without recurrent wound and graft sepsis was better than when treated locally or with partial graft removal. We therefore recommend removal of a thrombosed graft with an infected wound or an infected graft at the time of major limb amputation to decrease the incidence of wound complications and graft infection. Bony fragments Breakage of adhered scar with secondary infection Bony infection and Osteomyelitis
Stump infection with chronic discharging sinus for 8 months following amputation
There is extensive diffuse high signal in the vastusmedialis,intermedius and the lateralis and distal rectus femoris muscles. (also adductor magnus )Suspicious of muscle infection(pyomyositis). Poor outline of cortical margins of the femur in the distally (approximately 6 cm), some enhancement is seen alongespecially within the marrow on post gadolinium images A few low signal foci probably representing bony fragments There is probably a small collection at the end of the stump shown A small sinus tract is seen at the anterolateral aspect of the stump
After Re-fashioning of stump Immediately after surgery Recent Picture – healing by 2* intension
Good Surgical technique and Oedema management prevents stump infection De-bulk flap to give ideal stump shape which allows earlier casting Anterior beveling of tibia Allow for oedema in closure to prevent tension on suture line Interrupted skin closure to allow drainage Sutures not clips to allow for early compression Post operative management with early Compression stockinet (Not with skin clip) or Rigid Removable Dressing (RRD) Volume control Better wound healing Protection of stump (fall) Lowers the risk of knee contracture Reduces hospital stay and Prosthesis fitting time
Management Treat Stump infection early and prompt As it may lead to stump dehiscence and higher amputation It can cause serious systemic infection Delays the Prosthetic rehabilitation Prosthetic modification is immensely important for the holistic management.