Download
1 / 34
380 likes | 461 Vues
MACULAR DEGENERATION AND HEREDITARY RETINAL DYSTROPHIES. DR. SİNAN TATLIPINAR. ANATOMY. CLINICAL EVALUATION. Sx: -Decreased central vision, metamorphopsia, micropsia, macropsia Ancillary tests: -FFA: fundus fluorescein angiography, OCT: optical coherence tomography. AGE-RELATED MACULAR

E N D
MACULAR DEGENERATION AND HEREDITARY RETINAL DYSTROPHIES DR. SİNAN TATLIPINAR
CLINICAL EVALUATION • Sx: -Decreased central vision, metamorphopsia, micropsia, macropsia • Ancillary tests: -FFA: fundus fluorescein angiography, OCT: optical coherence tomography
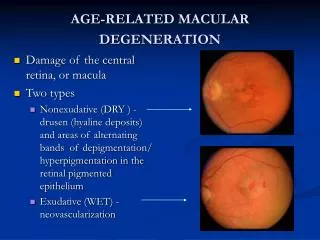
AGE-RELATED MACULAR DEGENERATION (AMD) 1. Atrophic AMD (Dry, nonexudative) 2. Exudative AMD • Choroidal neovascularization (CNV) -After 50 yr of age -AMD is the most common cause of visual loss in individuals over age 50. -Risk factors:Age, heredity, smoking
Drusen Histopathology Hard Soft • Larger, ill-defined spots • Small well-defined • spots • May enlarge and coalesce • Usually innocuous • Increased risk of AMD
`` FA of drusen Degree of hyperfluorescence depends on: • Extent of overlying RPE atrophy (window defect) • Amount of staining • Lipid content
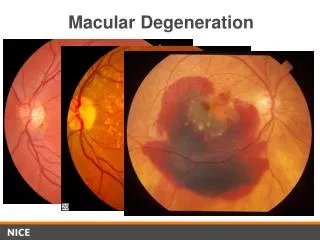
Drusen and AMD - progression Exudative AMD Atrophic AMD
Atrophic AMD Progression Initially drusen and non-specific RPE changes Late RPE (geographic) atrophy
Atrophic AMD Fluorescein angiogram Management Hyperfluorescence from RPE window defect Low-vision aids if appropriate
Choroidal neovascularization (CNV) • Less common than atrophic AMD but more serious • Metamorphopsia is initial symptom Suspicious clinical signs Subretinal blood or lipid Pinkish-yellow subretinal lesion with fluid
Angiographic classification of CNV Occult Well-defined (classical) • Extrafoveal > 200 m from centre of • FAZ • Poorly defined • Juxtafoveal < 200 m from centre of • FAZ • Obscured by PED, blood or exudate • Subfoveal - involving centre of FAZ
FA of classical CNV Leakage into subretinal space and around CNV Late staining Very early ‘lacy’ filling pattern
Possible subsequent course of CNV Subretinal (disciform) scarring Haemorrhagic sensory and RPE detachment Massive subretinal exudation Exudative retinal detachment
TREATMENT • ATROPHIC AMD: AREDS supplements • EXUDATIVE AMD: -Laser photocoagulation -Photodynamic Therapy -Intravitreal injection of anti-VEGF agents
OTHER ACQUIRED MACULOPATHIES 1. Central serous retinopathy 2. Idiopathic macular hole 3. Idiopathic premacular fibrosis 4. Cystoid macular oedema 5. Myopic maculopathy
Central serous retinopathy ( CSR ) • Self-limiting disease of young or middle-aged men • Usually unilateral • Localized, shallow detachment of sensory retina at posterior pole • Often outlined by glistening reflex
FA of central serous retinopathy (1) Smoke-stack appearance Early hyperfluorescent spot Later dye passage into subretinal space and vertical ascend Subsequent lateral spread until entire area filled
FA of central serous retinopathy (2) Ink-blot appearance - less common Early hyperfluorescent spot Subsequent concentric spread until entire area filled
Treatment of central serous retinopathy Most cases are self-limiting and do not require treatment Laser photocoagulation to RPE leak Post-treatment Pre-treatment • 4 months should elapse before considering treatment • Treatment induces resolution and lowers recurrence rate • Does not influence final visual outcome
Staging of idiopathic macular hole Stage 1a ( impending ) Stage 1b (occult) Normal fovea Stage 1a - ( impending hole ) Stage 1b - ( occult hole ) Dehiscence of photoreceptors Vitreous contraction with foveal detachment Stage 4 Stage 3 Stage 2 Seperation of cortex from retinal surface to form pseudo-operculum Complete vitreous separation Seperation of pseudo- operculum from edge of hole
Clinical features of full-thickness macular hole • Typically affects elderly females • Eventually bilateral in 10% • VA about 6/60 • Round punched-out area at fovea • Multiple yellow deposits within crater • Surrounding halo of sub-retinal fluid • Positive Watzke-Allen sign
Idiopathic premacular fibrosis Cellophane maculopathy Macular pucker • Severe retinal wrinkling and • vascular distortion • Opaque epiretinal membrane • Translucent epiretinal • membrane • May be associated with • macular pseudo-hole • Pucker emanating from • epicentre • Fine retinal striae and mild • vascular distortion
Cystoid macular oedema ( CMO ) Fluid-filled microcysts in outer plexiform and inner nuclear layer May lead to lamellar hole formation if longstanding
Important causes of CMO Retinal vein occlusion Background diabetic retinopathy Intermediate uveitis Post-cataract surgery
Clinical diagnosis of CMO • Loss of foveal depression • Retinal thickening • Yellow spot at foveola • Multiple cystoid areas
FA of cystoid macular oedema Late pooling with ‘flower-petal’ pattern Early parafoveal leakage Coalescence of leaking points
Myopic maculopathy Atrophic ‘Lacquer cracks’ • Large breaks in Bruch membrane • Progressive chorioretinal atrophy • May be associated with macular hole • Develop in about 5% of highly myopic eyes Macular haemorrhage Fuchs spot • Secondary pigment proliferation • From CNV with lacquer cracks • From lacquer cracks alone • Follows absorption of blood
Other fundus changes in myopia Tilted disc Posterior staphylomas Peripheral chorioretinal degeneration Lattice degeneration, holes and retinal detachment
HEREDITARY RETINAL DYSTROPHIES 1. Photoreceptor dystrophies • Retinitis pigmentosa • Retinitis punctata albescens • Fundus albipunctatus • Cone dystrophy • Leber congenital amaurosis 2. Retinal pigment epithelial dystrophies • Best vitelliform macular dystrophy • Adult best vitelliform macular dystrophy • Stargardt macular dystrophy • Fundus flavimaculatus • Familial dominant drusen • Sorsby pseudo-inflammatory macular dystrophy
Retinitis Pigmentosa 1. Inheritance • Sporadic (23%) • Dominant (43%) • Recessive (20%) • X-linked recessive (8%) • Uncertain (6%) 2. Presents- usually prior to 30 years 3. Prognosis- dominant best, x-linked worst 4. ERG- reduced
Progression of retinitis pigmentosa • Perivascular ‘bone-spicule’ • pigmentation • Fine dust-like pigmentation • Arteriolar attenuation • Initially mid-peripheral • Anterior and peripheral • spread • Optic disc pallor • Maculopathy • Unmasking of large • choroidal vessels
Ocular associations of retinitis pigmentosa Keratoconus (uncommon) Cataract (very common) Vitreous degeneration (common) Optic disc drusen (uncommon) Myopia (common) Open-angle glaucoma (uncommon
Atypical retinitis pigmentosa Quadrantic Sectorial Pericentric Paravenous