Download

1 / 10
150 likes | 670 Vues
MITRAL STENOSIS. Dr R Schulenburg Division of Adult Cardiac Surgery, Universitas Hospital, BFN. Etiology and Essential Pathology. Predominately post-inflammatory scarring(other malignant carcinoid, SLE) Fibroreactive transformation of the valve

E N D
MITRAL STENOSIS Dr R Schulenburg Division of Adult Cardiac Surgery, Universitas Hospital, BFN
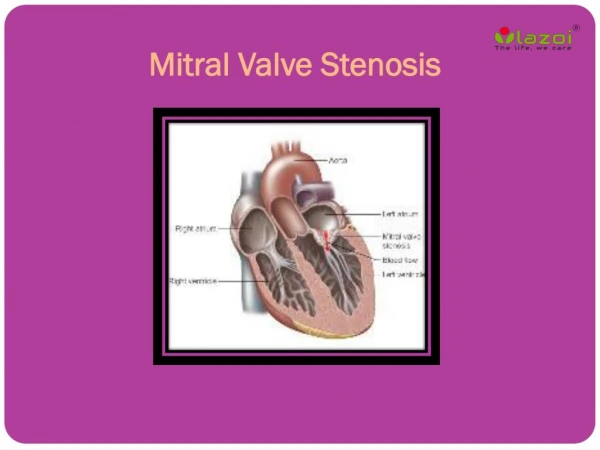
Etiology and Essential Pathology • Predominately post-inflammatory scarring(other malignant carcinoid, SLE) • Fibroreactive transformation of the valve • Affecting all segments of the valvular apparatus • Calcifications at commisural edges lead to classic ‘fish-mouth’ appearance • Only 25% have pure MS
Pathophysiology • Reduction in MVA with a rise in atrioventricular gradient • LA hypertrophy and imposes a pressure load on the RV through the development of pulmonary hypertension • Increases in RV end-diastolic pressure and volume cause RV dilatation which may result in funtional TVR(annular dilatation)
Pathophysiology • LV diastolic function is usually preserved although there may be(25%) dysfunction in patients with severe, chronic MS(chronic preload reduction and/or extension of scarring from the valve to adjacent myocardium) • Systemic effects of severe TVR
Classification and Natural History • Mild(MVA>1.5, MG<5mmHg, PASP<30mmHg) • Moderate(MVA 1-1.5, MG 5-10mmHg, PASP 30-50mmHg) • Severe(MVA<1, MG>10mmHg, PASP>50mmHg)
Natural History • MV>1.5 usually does not produce symptoms at rest • Symptoms develop when the LAP increases(Dyspnoea) >5mmHg • Occurs when there is an increase in transmitral flow or a decrease in diastolic filling time(exercise, emotional stress, infection, pregnancy, AF with a rapid ventricular response)
Nutural History • MS is a continuous, progressive, life-long disease, usually consisting of a slow, stable course in the early years followed by a progressive acceleration in later life • Once symptoms develop, there is another period of almost a decade before symptoms become disableing • Asymptomatic/minimally symptomatic: survival is 80% at 10yrs but once significant limiting symptoms develop, there is a dismal 0-15% 1-year survival rate
Natural History • When severe pulmonary HPT develops , mean survival drops to <3yrs • 60-70%-progressive pulmonary and systemic congestion • 20-30%-systemic embolism • 10%-pulmonary embolism • 1-5%-infection
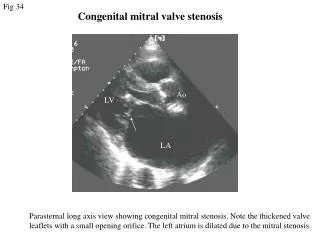
Diagnosis • History: slow, indolent increase in dyspnoea and general fatigue(any sudden change in symptom complex should raise suspicion!) • Clinical:RV heave, Apex beat, Diastolic rumble, Opening snap • ECG • CXR:Cardiac chamber enlargement, Pulmonary venous hypertension, Pulmonary arterial hypertension • ECCHO/TEE • Cardiac cath
Management • Medical: AB prophylaxis, diuretics, negetive chronotropic drugs, atrial fibrillation • Interventional: Percutaneous balloon valvotomy • Surgical: Cosed/open commissurotomy, MVR