Download
1 / 22
220 likes | 486 Vues
The Topical Management of Psoriasis. Alexandra Pyle Bsc (Hons) Registered Nurse. What is Psoriasis?. Psoriasis is a chronic inflammatory skin disorder characterised by thickened, scaly plaques. Causes of Psoriasis. There is no definite cause for Psoriasis

E N D
The Topical Management of Psoriasis Alexandra Pyle Bsc (Hons) Registered Nurse
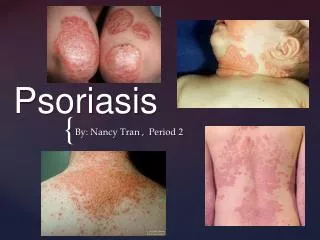
What is Psoriasis? Psoriasis is a chronic inflammatory skin disorder characterised by thickened, scaly plaques
Causes of Psoriasis There is no definite cause for Psoriasis But two factors that can contribute to the development of psoriasis are: A Genetic Predisposition Direct injury to the skin (knoeber Phenomenon)
Triggers include • Infection (streptococcal sore throat) • Drugs / medications • Stress • Smoking • Alcohol (to excess) • Climatic changes
7 Types of Psoriasis • Chronic Plaque Psoriasis • Scalp Psoriasis • Guttate Psoriasis • Flexural Psoriasis • Localised Pustular Psoriasis • Generalised Pustular Psoriasis • Erthrodermic Psoriasis
Treatments • Treatment choices include: • Step 1 Topical therapy • Step 2 Phototherapy • Step 3 Systemic therapy • Step 4 Biologics
Emollients • Moisturise dry skin, diminish desire to scratch, and reduce need for topical therapies • Creams; Dermol 500, Diprobase, Cetomacrogol. Hydromol, Aveeno. • Ointments; 50:50 WSP, Epaderm/Hydromol, emulsifying ointment
Coal Tar • One of the oldest and most widely used treatments • Slows rapid proliferation of skin cells and restores skin appearance • Reduces inflammation, itching and scaling • Applied directly to the skin • Strengths 2%, 5% and 10% • New strength patch tested approx every 3 days
Dithranol • Effective remedy for psoriasis lesions, used for many years • Dithranol accumulates in mitochondria where it interferes with the supply of energy to the cell, probably by oxidation releasing free radicals. This impedes DNA replication and so slows the excessive cell division that occurs in psoriatic plaques. In addition Dithranol may act by reducing the elevated levels of cGMP that occurs in psoriasis. Applied directly to skin plaques • Strengths 0.1% to 15% • Dose gradually increased as resistance is built up • Can cause irritation and discolouration of skin not affected by psoriasis
Vitamin D Analogues • Calcipotriol (dovonex) BD • Calcitriol (Silkis) BD • Tacalcitriol (Curatoderm) OD • Dovobet –combines strong steroid with dovonex • Work well to clear psoriasis • Have few side effects
Phototherapy • Skin exposed to wavelengths of ultraviolet light • 2 types available – UVA and UVB • Treatment with UVA is helped by taking tablets known as psoralens – known as PUVA therapy
Tablet / Systemic therapy • Neotigason (Acitretin) – once daily • Ciclosporin – once daily • Methotrexate – once weekly • Mycophenolate mofetil – once daily
Biologic Therapy These are antibodies or receptor blockers to TNF alpha Given via intravenously or subcutaneous administration and multiple dose Main problems increased risk of infections, antibody formation, expense of the drug
Dermatology Day Care Unit • Provides application of topical therapies • Provides support and education • Long stay patients can have more than 1 topical applications • Encourages self management of psoriasis • Difficult to reach areas can be treated • e.g. Back, scalp, feet