Download
1 / 42
430 likes | 495 Vues
Oxidative Stressmarker als Frühdiagnostik für Demenz in Vienna Transdanube-Aging "VITA" Projekt. Dr. Grünblatt E., Würzburg University, Clinic for Psychiatry. Vienna-Transdanube-Aging VITA.

E N D
Oxidative Stressmarker als Frühdiagnostik für Demenz in Vienna Transdanube-Aging "VITA" Projekt Dr. Grünblatt E., Würzburg University, Clinic for Psychiatry.
Vienna-Transdanube-Aging VITA eine prospektive, bevölkerungsbezogene, interdisziplinäre Kohortenstudiezur Vorhersage der Alzheimer Demenz LBI für Altersforschung, Wien
Population der VITA-Studie ... ... sind alle österreichischen Einwohner des 21. und 22. Wiener Gemeindebezirks, deren Geburtstag zwischen Mai 1925 und Juni 1926 (N=1920) liegen. LBI für Altersforschung, Wien
SMZ-O Vienna Transdanube Aging VITA Alle 75-jährigen Einwohner der Bezirke 21 und 22
Studienverlauf 2000 2001 2002 2003 2004 2005 2006 2007 2008 Basisuntersuchung 1. Follow Up 2. Follow Up
Interdisziplinäres Untersuchungsdesign der VITA bei der Hauptuntersuchung • Blutabnahme- Blutchemie, Genetik • Anamnese- Krankheiten, Medikamente, Psychosoziale & Körperliche Aktivitäten, Bildung, Beruf, Familienstand, Ernährung, Alkohol, Nikotin,…. • Fremdanamnese-CDR, ADL, IADL,…. • Neuropsychologische Untersuchung- CERAD-Batterie, Konzentartionstest, Sprachtests,…. • Psychiatrische Untersuchung- Demenz nach DSM-IV, NINCDS-ADRDA, AIREN, Depression (DSM-IV), Angst,…. • Neurologische Untersuchung- Insult, Parkinson,….. • Bildgebende Verfahren- Magnetresonanztomographie, PET der MCI-Verdachtsfälle und Demenz-Fälle
Basisuntersuchung: Teilnehmerrate Alterskohorte im 21. und 22. Bezirk N=1920 lt. Wahlbehörde KONTAKT N=1505 (100%) Nur Voruntersuchung N=31 (2%) Absage N=808 (54%) TEILNAHME N=697 (46% der kontaktieren Probanden) Telefoninterview N=60 (4%) Interesselosigkeit N= 410 Krankheit N= 223 Zeitmangel N= 67 Negativismus N= 49 Angst N= 30 Depression N= 17 Vergesslichkeit N= 12 Untersuchungstag N=606 (40%)
VITA: 1. Follow-UpStand: 30.4.2005 1. Nachuntersuchung eingeladen wurden zum geplanten Termin bis 30.04.2005: N=587 (97% der 606 Probanden) Verstorben N=36 (6,1%) Absage N=66 (11,2%) Kontaktiert N=551 Telefoninterview N=10 (1,7%) Erkrankung N= 32 Kein Interesse N= 25 Zeitmangel N= 3 Angst N= 3 Depression N= 1 Vergesslichkeit N= 1 Angeh. lehnt ab N= 1 Teilnahme N=477 (81,3%) Hausbesuch N=18 (3,1%) Untersuchungstag N=449 (76,5%)(4KT) in Evidenz N=8 (1,4%)
Zwischenstand der ersten Follow-Up der VITA Probanden mit depressiven Syndromen (major, minor, subsyndromaler Depression) : n = 178 (43 %) Probanden, die kognitiv deutlich schlechter wurden n = 105 (26 %) 47 (11 %) 58 (14 %) 120 (29 %) 186 (45%) Probanden, die mit 78 Jahren weder dement noch depressiv waren n = 186 (45 %)
Centenarian-Projekt • Untersuchst chronische betreute alte Patienten leiden an verschiedenen Demenz Typ • Durchschnitt Alter= 81 Jahre (52 bis 103 Jahre; n=185)
„Mild Cognitive Impairment“Petersen et al. 1995, 2001 • international anerkanntes Konzept zur Erfassung der Alzheimer Demenz im frühen Stadium • Kriterien: • Subjektive Vergesslichkeit (1995) des Betroffenen und/oder Bericht eines Angehörigen über Gedächtnisprobleme (2001) • beeinträchtigte Gedächtnisleistung (1.5 SD unter dem Mittelwert der altersentsprechenden Population) • andere kognitive Leistungen im Normbereich • keine beeinträchtigten Aktivitäten des täglichen Lebens • keine Demenz
Consensus-Meeting: General Criteria for MCI(Winblad et al. 2004, J Int Med, 256) • not normal, not demented (does not meet criteria – DSM IV, ICD 10 – for a dementia syndrome) • cognitive decline - self and/or informant report and impairment on objective cognitive tasks and/or - evidence of decline over time on objective cognitive tasks • preserved basic activities of daily living / minimal impairment in complex instrumental functions
Operationalisierung der MCI Kriterien in der VITA • DMS-IV Kriterien für Demenz nicht erfüllt • MMSE größer gleich 24 • Activities of Daily Living (ADL) (nach Lawton et al, 1969): 29, 30 • 6 psychometrische Verfahren (jeweils 1.5 SD) • CERAD Wortliste abrufen (Gedächtnis) • CERAD Konstruktive Praxis abrufen (Gedächtnis) • CERAD Wortflüssigkeit • CERAD Benennen • CERAD Konstruktive Praxis • Trail-Making Test (TMT)-B Geteilte Aufmerksamkeit
Stand der MCI-Forschung • Welche Variablen sagen die Konversion zu den verschiedenen Demenzen (AD, LBD, VD, FTD) voraus (Sensitivität, Spezifität) • MRI medial temporal atrophy (Korf et al, 2004; ...) Diffusion weighted MRI (Kantarci et al,2005) Spektroskopie (Modrego et al, 2005; ...) • PET par-temp. AD-muster (Chetelat et al, 2005;..).. • Liquor Aß42, Tau (Hampel et al, 2004; ...) • APOE Epsilon4 Allel (Farlow et al, 2004) • Serum Oxidative Stress (Beal, 2005), ... • .........................
VITA- Projekt: Frühdiagnose der DAT • Objektiv: Frühdiagnose der Alzheimer Krankheit und andere Demenzsyndrom mit Molekularmarker im Blutzellen
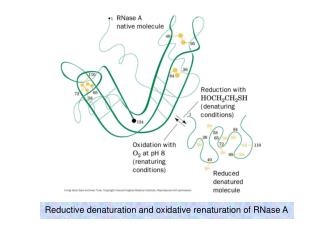
Pathogenese des oxidativen Stress Definition für oxidativen Stress: „A disturbance in the prooxidant-antioxidant balance in favor of the prooxidant, leading to potential damage“ Sauerstoffradikale: sind unstabil und sehr reaktiv • Das Gehirn ist empfindlich für oxidativen Stress weil: • niedrige Spiegel von Glutathion • höhere Spiegel von polyunsaturated fatty acids • hoher Sauerstoffverbrauch O2 • Neuronen sind postmitotisch (Ablagerung von Beschädigung) • höhere Spiegel von Eisen und Amyloid Plaques
Biomarker Oxidative Stressmarker in Blutzellen zur Frühdiagnostik • platelet MAO (MAOB) • erythrocyte Cu/Zn-SOD (SOD1) • plasma lactoferrin (LTF)
H2O2 • platelet MAO-B: • human platelets contain only MAO-B • activity is very stable • activity increases in AD • low activity is associated with behavior/smoking H2O MAO-B Hydrogen Peroxyde + NH3 O2 Dopamin Pathogenesis- MAO-B • localized in the outer mitochondrial membrane • catalyzing the oxidative deamination of catecholamines • MAO-A: serotonin (5-HT), norepinephrine CLORGYLINE • MAO-B: phenylethylamine, dopamine SELEGILINE • producing H2O2
O2- Superoxide Fe3+ iron O2-+Fe3+O2+Fe2 O2-+1e-+2H+H2O2 H2O2+Fe2+OH•+OH-+Fe3+ OH• Hydroxyl radical Haber-Weiss reaction H2O2 H2O O H O H MAO-B Hydrogen Peroxyde + NH3 HOH O2 Dopamin Pathogenese des oxidativen Stress DNA,RNA Proteins Lipids C
Biomarker Oxidative Stressmarker in Blutzellen zur Frühdiagnostik • platelet MAO (MAOB) • erythrocyte Cu/Zn-SOD (SOD1) • plasma lactoferrin (LTF)
2H+ H2O O2- O2- H2O Superoxide Superoxide O2 H2O2 • erythrocyte Cu/Zn-SOD: • erythrocytes contain only Cu/Zn-SOD • activity AD increased/decreased ? SOD Catalase Glutathione Peroxidase Hydrogen Peroxyde Pathogenesis-Cu/Zn-SOD • first line of defence against reactive oxigen spiecies (ROS) • three forms: Cu/Zn-SOD, Mn-SOD, Fe-SOD • mutation in ALS
O2- Superoxide Fe3+ iron O2-+Fe3+O2+Fe2 O2-+1e-+2H+H2O2 H2O2+Fe2+OH•+OH-+Fe3+ OH• Hydroxyl radical Haber-Weiss reaction H2O2 Glutathione Peroxidase Catalase SOD Hydrogen Peroxyde H2O O2 H2O Pathogenesis-Oxidative stress DNA,RNA 2x + 2H+ Proteins Lipids
Biomarker Oxidative Stressmarker in Blutzellen für Frühdiagnostik • platelet MAO (MAOB) • erythrocyte Cu/Zn-SOD (SOD1) • plasma lactoferrin (LTF)
lactoferrin Fe3+ iron • plasma lactoferrin (LTF): • amount in AD ? Pathogenesis- Lactoferrin • glycoprotein • belongs to transferrin-family • binds iron more tightly than transferrin • iron chelator antioxidant • found in neurodegenerative disease brains
O2- Superoxide Fe3+ Fe3+ iron iron O2-+Fe3+O2+Fe2 O2-+1e-+2H+H2O2 H2O2+Fe2+OH•+OH-+Fe3+ lactoferrin lactoferrin OH• Hydroxyl radical Haber-Weiss reaction H2O2 Hydrogen Peroxyde Pathogenese des oxidativen Stress DNA,RNA Proteins Lipids
MAO-B Aktivität in erster Rekrutierung der VITA-Studie 1 1 ,9 ,9 ,8 ,8 ,7 ,7 ,6 ,6 ,5 MAOB activität (nmol/mg protein*min) ,5 ,4 ,4 ,3 ,3 ,2 ,2 N=523 N=523 N=15 N=18 N=48 N=15 ,1 ,1 0 0 -,1 -,1 Gesund Vascular DAT Mix Gesund Dement ANOVA, p=0.096 ANOVA, p=0.279
1 ,9 ,8 ,7 ,6 ,5 ,4 MAOB Aktivität (nmol/mg protein*min) ,3 ,2 ,1 0 -,1 16 18 20 22 24 26 28 30 32 MMSE Korrelation zwischen MAO-B Aktivität und Mini-Mental-State-Examination (MMSE) R^2 = 4.507E-4 (ANOVA p=0.613) MAO-B Aktivität ist nur tendenziell erhöht bei niedrigerem MMSE-Score
MAO-B Aktivität: VITA-Studie vs. Centenarian-Projekt .6 .5 .4 .3 MAO-B activität (nmol/mg protein*min) .2 n=129 n=297 .1 0 -.1 Centenarian VITA • platelet MAO-B Aktivität erhöht bei Demenz (Centenarian) • ANOVA: p<0,0001S
.6 .5 .4 .3 MAOB activität (nmol/mg protein*min) .2 .1 0 -.1 -5 0 5 10 15 20 25 30 35 MMSE Korrelation zwischen MAO-B Aktivität und MMSE mit VITA & Centenarian Centenarian VITA MAOB activität (nmol/mg protein*min) = .229 - .004 * MMSE; R^2 = .162 P<0.0001 MAO-B Aktivität ist signifikant erhöht in niedrigere MMSE
,25 ,2 ,15 ,1 MAOB Aktivität (nmol/mg protein*min) ,05 0 -,05 MAO Aktivität und MAO-B intron 13 polymorphism in VITA AA GA N=45 GG N=19 N=22 N=21 N=21 Männer Frauen
MAO-B Aktivität: Effekt des Rauchens 1 ,9 ,8 ,7 ,6 ,5 MAOB Aktivität (nmol/mg protein*min) ,4 ,3 ,2 N=324 N=247 ,1 0 -,1 Raucher Nicht Raucher Rauchen reduziert MAO-B Aktivität (p=0.077)
Erythrocyten SOD (SOD1) Aktivität in erster Rekrutierung der VITA-Studie 1,2 1 ,8 ,6 SOD Aktivität (U/µg protein) ,4 N=481 N=16 N=14 N=16 ,2 0 -,2 Gesund DAT Mix Vascular
1,2 1 ,8 ,6 SOD Aktivität (U/µg protein) ,4 ,2 0 -,2 16 18 20 22 24 26 28 30 32 MMSE Korrelation zwischen SOD Aktivität und MMSE-VITA Studie R^2 = 0.003 (ANOVA p=0.1755) SOD Aktivität ist tendenziell niedriger bei niedrigerm MMSE
1.2 1.2 1 P<0.005 Männer 1 .8 SOD activität (U/µg protein) .8 .6 Frauen SOD activität (U/µg protein) .6 .4 .4 N=191 .2 N=88 .2 0 Centenarian VITA 0 Centenarian VITA SOD Aktivität in VITA-Studie vs. Centenarian-Projekt P<0.005 N=117 N=74 N=22 N=66 SOD Aktivität ist signifikant niedriger in Centenarian (Demenz), speziell bei Frauen
1,2 1 ,8 Centenarian SOD Aktivität (U/µg protein) ,6 VITA ,4 ,2 0 -5 0 5 10 15 20 25 30 35 MMSE SOD activity (U/µg protein) = ,264 + ,003 * MMSE; R^2 = ,023 Korrelation Zwischen SOD Aktivität und MMSE: VITA & Centenarian Bartlett-Test P<0.05 SOD Aktivität signifikant erniedrigt bei niedrigerem MMSE
11 10 9 8 7 6 5 4 3 2 1 0 20 21 22 23 24 25 26 27 28 29 30 31 Plasma lactoferrin: VITA-Studie 12 10 8 6 LTF plasma Spiegel N=1 4 N=5 N=4 N=48 2 0 -2 Mix Vascular DAT Gesund MMSE R^2 = 0.017 (ANOVA p=0.3361) Bei DATtendiert Lactoferrin erniedrigt zu sein (ANOVA p=0.32)
12 12 10 10 8 8 LTF 6 6 LTF Plasma Spiegel 4 4 2 2 0 0 -5 0 5 10 15 20 25 30 35 Centenarian VITA MMSE Plasma Lactoferrin Spiegel in VITA-Studie vs. Centenarian-Projekt LTF = 2.143 + .018 * MMSE; R^2 = .014 In Cenetnarian (Demenz) LTF Spiegel tendiert erniedrigt zu sein
Conclusions • Only small (insignificant) trends towards an association between oxidative stress and cognition in the context of a community-based study at age 75 • Longitudinal observations will help to prove whether oxidative stress related markers will help to predict cognitive decline and Alzheimer dementia in the VITA study.
VITA-Team LBI für Altersforschung, Wien
DANKE University of Würzburg, Clinic of Psychiatry and Psychotherapy, Würzburg, Germany Prof P. Riederer Dr. E. Koutsilieri R. Schlöber M. Fischer J. Li M. Hofmann Ludwig Boltzmann Institute for Aging Research, Vienna, Austria Prof. KH Tragl Mag. S. Weissgram Fr. U. Laure Prof. W. Danielczyk Dr. N. Moustafaie Fr. T. Stelzhammer Prof.. P. Fischer Dr. W. Krampla Prof. KA Jellinger Prof. Dr. P. Bauer Mag. S. Jungwirth Dr. S. Torma Dr. K. Huber Doz. Dr. G. Hinterberger Geriatric Centre `Wienerwald', Vienna, Austria Dr. N. Sterba Dr. W. Adamcyk Dr. B. Dittrich Dr. F. Müller Dr. K. Oberegger Dr. I. Wichart Dr. G. Gatterer Für das hilfsmittel für VITA Studie