Download
1 / 12
120 likes | 425 Vues
Severe recurrent corneal calcification following autologous submandibular gland translocation . RM Santaella MD, HT McGee MD, WD Mathers MD Department of Ophthalmology Oregon Health & Science University Portland, OR. Abstract:

E N D
Severe recurrent corneal calcification following autologous submandibular gland translocation RM Santaella MD, HT McGee MD, WD Mathers MD Department of Ophthalmology Oregon Health & Science University Portland, OR
Abstract: • Purpose: To report severe recurrent corneal calcification as an adverse effect following translocation of autologous submandibular gland and to identify factors that may contribute to the development of this effect. • Methods: Case report • Case: 84 y.o. female with severe dry eye and persistent epithelial defect underwent autologous submandibular gland translocation to the right eye. Excellent ocular surface moisture was achieved, however, the patient developed severe corneal calcification requiring penetrating keratoplasty. This calcification then rapidly recurred in the corneal graft. • Conclusion: Recurrent and difficult to treat calcific band keratopathy may result following otherwise successful autologous submandibular gland transplantation as treatment for dry eye.
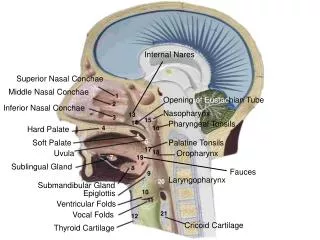
Introduction: • Autologous transplantation of the submandibular salivary gland has been previously described for treatment of severe, refractory dry eye1. • While effective at providing moisture to the ocular surface, the procedure can lead to irregular tear production and overflow tearing2. • Calcific band keratopathy occurs when calcium salts, primarily in the form of hydroxyapatite, are deposited in the superficial layers of the cornea. • This deposition has been described in several systemic as well as local ocular disorders3. • To our knowledge, however, this is the first report of severe recurrent corneal calcification following salivary gland redirection.
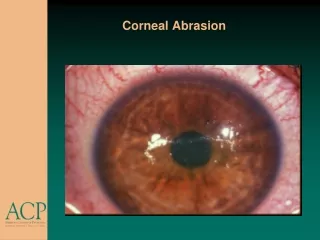
Case: • An 84 year old caucasian female with severe dry eye and filamentary keratitis underwent a submandibular gland redirection procedure as an adjuvant treatment for an epithelial defect in her right eye which had been persistent for 5 months. • During her 2 week postoperative visit she was noted to have developed significant band keratopathy in the area of the persistent epithelial defect (Figure 1). Moisture from the salivary gland redirection was very good. • A penetrating keratoplasty was performed to restore a healthy ocular surface. • At the 1 week visit a small epithelial defect was noted. • At 2 weeks, dense calcification was again noted on the transplanted graft with the area of the epithelial defect being affected most (Figure 2). • Chelation using EDTA performed 1 month after the corneal transplantation was unsuccessful. • A repeat systemic workup (and review of previous labs) for band keratopathy was unremarkable. • A second corneal transplant was required 1 month after the first graft due to corneal melting. • A total epithelial defect was noted the 1st post operative day, and recurrent calcification was noted again on the 2nd postoperative day.
Figure 1: Severe band keratopathy noted 2 weeks after submandibular gland transplantation. The dense inferior portion corresponds to the area of prior epithelial defect. Figure 3. Histopathology of recipient corneal button showing calcific deposits beneath Bowman’s membrane in contrast to typical band shaped keratopathy. Hematoxylin and eosin stain (A) and alizarin red (B). AB
Figure 2: Recurrent band keratopathy 2 weeks after corneal transplantation. Figure 3. Histopathology of corneal button showing sharply demarcated calcific deposits replacing Bowman’s layer and penetrating into superficial stroma in an area of epithelial defect. Hematoxylin and eosin stain (A) and alizarin red (B). AB
Discussion: • Band-shaped keratopathy (BSK) has been described in association with several factors, including systemic disorders usually associated with calcium phosphate metabolism, uveitis, use of pilocarpine with mercurial preservatives, viscoelastics, and intraocular silicone oil3-8. • Calcification in BSK has been described to occur at the level of Bowman’s membrane (Bowman 1849). • The calcium in BSK can build in the subepithelial space to the point where it disrupts the epithelium, but that is usually a late finding. • Rapid calcium deposition has been described in association with epithelial defects and corneal grafts in conjunction with the use of topical eye medications containing phosphates or phosphate buffered solutions3-4, 9-12. • The calcification noted in this patient appears to be similar to the more rapid deposition associated with topical phosphate containing medications and epithelial compromise. • This patient had been on preparations of prednisolone acetate and timolol that both contained phosphates among their inactive ingredients: EconoPred (Prednisolone acetate 1%) and Timolol 0.5% both manufactured by Alcon Laboratories, (Fort Worth, TX). However, the calcification recurred despite discontinuation of these phosphate containing medications and repeat corneal transplantation. • We believe that this patient’s salivary gland redirection played a major role in the calcification process.
Table 1. Inorganic chemistry of saliva, tears, and serum Discussion: • The difference in pH, calcium and phosphate concetrations are key features that contributed to the severe calcification seen in this patient. • Tears have a lower calcium concentration than saliva or serum13-15 and, while there is no direct association between serum calcium concentration and tear concentration16, relatively minor disturbances, such as those seen in renal failure, can result in significant calcium deposition such as BSK. • Saliva from the submandibular gland, usually has much higher concentrations of both calcium and phosphate than are found in lacrimal gland tear secretions13,17. (see Table 1) • The pH of saliva and submandibular gland secretions is also lower than that of the tear film13-15.
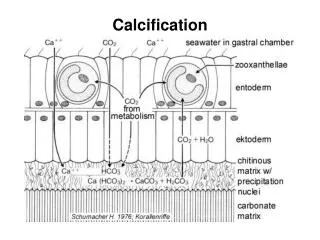
Discussion: • Saliva protects teeth from dissolution18. • This is accomplished by bathing teeth in a supersaturated solution with respect to the minerals which compose teeth13,15. • Hydroxyapatite and other forms of apatite are the major constituents of teeth. • In the cornea, calcium deposition also typically occurs as hydroxyapatite9. • The balance between dissolution and precipitation is governed by the dissociation equilibrium of hydroxyapatite. • This equilibrium is dependent on the concentrations of ions in solution. • In the case of hydroxyapatite (Ca10(PO4)6(OH)2) these ions are calcium, phosphate and hydroxide. • However, the dissociation equilibrium of hydroxyapatite is very sensitive to pH. • In the mouth a critical pH of 5.2 has been found in which a pH higher than 5.3 tends to lead to precipitation of tooth enamel and lower than 5.2 leads to tooth dissolution13. Figure 4. The dissociation equilibrium equation for calcium hydroxyapatite
Discussion: • The association of corneal exposure and the interpalpebral location of BSK has been well described20. Increased tear evaporation leading to an increase in tonicity and ion concentration within the tear film is a factor that also plays a role in the dissociation equilibrium shifting the equilibrium towards precipitation. • Exposure can also lead to epithelial barrier dysfunction and breakdown exposing a direct access to Bowman’s membrane. This direct access to Bowman’s membrane may be a factor in the speed at which calcification occurs. • Our patient had full eyelid closure and was treated with aggressive lubrication with ointment and despite the lubrication efforts she developed severe calcification. • This patient was treated with oral pilocarpine hydrochloride (Salagen, MGI Pharma) at 5mg PO three times a day throughout the time course of her corneal calcification. Perhaps this medication may have also contributed in the development of her condition by increasing the amount of secretions or perhaps the composition of the submandibular saliva. However, a study measuring change in the salivary constituents on patients with graft versus host disease treated with pilocarpine showed no change in the calcium or phosphate concentrations21.
Conclusions: • There are several variables that may contribute to corneal calcification in the setting of submandibular gland transplantation as treatment for severe dry eye, including calcium and phosphate concentrations, pH, tonicity, epithelial disruption, and degree of tear evaporation. • Dense corneal calcification is a severe and difficult to manage complication that may arise after autologous transplantation of the submandibular salivary gland for dry eye.
References: • Geerling G, Sieg P, Bastian GO, Laqua H. Transplantation of the autologous submandibular gland or most severe cases of keratoconjunctivitis sicca. Ophthalmology 1998; 105: 327-335. • Leibovitch I, Hoyama E, Limawararut V, Crompton J, Selva D. Novel technique to control hypersecretion from a transplanted autologous submandibular salivary gland for keratoconjunctivitis sicca. Cornea 2006; 25: 1251-53. • Smolin G. Dystrophies and degenerations. In: Smolin G, Thoft RA. The Cornea. 2nd ed. Boston, Mass:Litle Brown & Co. 1989:429. • Kennedy RE, Primitive RD, Landers PM. Atypical band keratopathy in glaucomatous patients. Am J Ophthalmol. 1971;72:917-922 • Coffman MR, Mann PM. Conreal subepithelial deposits after use of sodium chondroitin. Am J Ophthalmol. 1986;102:276. • Nevyas AS, Raber IM, et al. Acute band keratopathy following intracameral Viscoat. Arch Ophthalmol. 1987;105:958. • Binder PS, Deg JK, kohl FS. Calcific band keratopathy after intraocular chondroitin sulfate. Arch Ophthalmol. 1985;105:1243. • Sternberg P Jr., Hatchell DL, et al. The effect of silicone oil on the cornea. Arch Ophthalmol. 1985;103:90. • Taravella MJ, Shulting RD, MAder TH, et al. Calcific band keratopathy associated witht the use of topical steroid-phosphate preparations. Arch Ophthalmol. 1994;112:608-613. • Bernauer W, Thiel MA, et al. Corneal calcification following intensified treatment with sodium hyaluronate articial tears. Br J Ophthalmol. 2006;90:285-8. • Daly M, Tift SJ, Munro PM. Acute corneal calcification following chemical injury. Cornea 2005; 24:761-765. • Schlötzer-Schrehardt U, Zagorski Z, Holbach LM, et al. Corneal stroma calcification after topical steroid-phosphate therapy. Arch Ophthalmol 1999; 117:1414-1418. • Larsen MJ, Pearce EIF. Saturation of human saliva with respect to calcium salts. Arch Oral Biol 2003; 48:317-322. • Van Haeringen NJ. Clinical biochemistry of tears. Surv Ophthalmol. 1981; 26:84-96. • Cummings CW, Haughey BH, Thomas JR, Harker LA, Flint PW. Composition of saliva. In: Cummings: Otolaryngology: Head & Neck surgery, fourth edition. Mosby, Inc. 2005. • Avisar R, Savir H, Sidi Y, Pinkhas J. Tear calcium and magnesium levels of normal subjects and patients with hypocalcemia or hypercalcemia. Invest Ophthalmol. 1977; 16: 1150-1151 • Tsubota K, Higuchi A. Serum application for the treatment of ocular surface disorders. Int Ophthalmol Clin. 2000; 40:113-122. Review. • Zero DT, Lussi A. Erosion-- Chemical and biological factors of importance to the dental practitioner. Int Dent J 2005; 55:285-290. • Fosdick LS, Starke C, Jr. Solubility of tooth enamel and saliva at various pH levels. J Dent Res 1939; 18:417-430. • O’Connor GR. Calcific band keratopathy. Trans Am Ophthalmol Soc. 1972; 70:58-85. • Nagler R. The effect of pilocarpine on salivary constituents in patients with chronic graft versus host disease. Arch Oral Biol 2001; 46:689-695.