Download
1 / 36
360 likes | 493 Vues
CORE. Managing care provision for patients with mental disorders under NHS conditions in the UK Stuttgart, March 2002. CORE. C linical O utcomes in R outine E valuation. Scientific & Service Partners. Authors Michael Barkham Chris Evans

E N D
CORE Managing care provision for patients with mental disorders under NHS conditions in the UK Stuttgart, March 2002
CORE • Clinical • Outcomes in • Routine • Evaluation
Scientific & Service Partners Authors Michael Barkham Chris Evans Frank Margison John Mellor-Clark Janice Connell Chris Leach Mike Lucock
Primary Funders • Mental Health Foundation • Counselling in Primary Care Trust
NHS Implementation Programme • By end March 2001: HA should have in place protocols agreed and implemented between primary and specialist mental health services for the management of depression, anxiety disorders, ….. those requiring psychological therapies • By end March 2002: all HA should have reviewed these protocols to ensure they are being used and operating effectively.
How the NHS is organised • Primary and secondary care • Primary Care Trusts now commissioners of services • Secondary care and primary care have psychological therapies • Severe, enduring mental illness a key target • Poor implementation of psychological treatments for severe disorders
NHS initiatives • National Service Frameworks (one for mental health) • Local Implementation teams • Definite targets and priorities • Care Programme Approach • Suicide Prevention • New neuroleptics (NICE)
Initiative meltdown!! • Integration of health and social care (new Health and Social Care Trusts) • Clinical and service governance • R&D re-organisation of funding • Appraisal • Guidelines • and Outcomes monitoring!
Complementary paradigms Evidence-based Practice Practice-based Evidence
Efficacy studies Randomised Controlled Trials Evidence-based practice as policy Practitioners Practice-based evidence Effectiveness studies Routine Clinical Treatment Practitioners
Practice-based research • Logic, feasibility and plausibility should govern planning, data collection, and interpretation • Basic tenets of measurement remain: • validity, reliability, control of bias • completeness of data
Requirements of a “core” measure • Pragmatic and user-friendly • Acceptable psychometric properties • Implementation on a broad basis • Computer-scannable • Co-ordinating centre • Extensions to other domains
What is the CORE-OM? • 34 items on two sides of A4 • tick box completion • five response levels (0 to 4) • pan-theoretical (“CORE”) • simple language • hand scorable • computer scannable • short forms available
CORE-System Practitioner Patient CORE Therapy Assessment Form Referral, support systems, use of services, medication, identified problems, risk, patient coping strategies CORE-OM CORE-SF A/B/A/B CORE End of Therapy Form Type of therapy, frequency, ending, risk, identified problems, benefits of therapy, change in medication CORE-OM
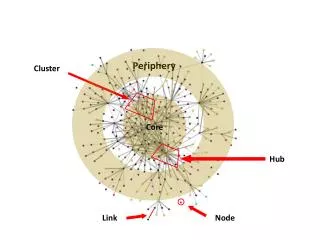
Hub & Spoke Problem-specific core batteries Referential measures CORE
What does it measure? • Four domains covered • Subjective well-being • Social functioning • Problems/symptoms • Risk • to self (harm/suicide) • to others • Eight items positively keyed • Mixture of high and low threshold items
CORE-Support On site hand scoring CORE-OM PC On site data mounting & analysis CORE Team comprehensive analysis of CORE System Service Provider CORE Team processing of CORE-OM
CORE Family of Measures CORE-OM Adults Older Adults Translations CORE-GP General Population Teen-CORE Adolescents Kiddy-CORE Children
CORE Implementation T I M E C O R E-Short Form CORE-OM S E V E R I T Y CORE-Non Risk CORE-GP
Severity Pre-therapy Time Post-therapy
Current work I • CORE-GP CORE for the general population. 14 items (risk and high-level items removed) • Students, n=6000 • Compares well to GHQ-12 (.85 correlation) • Use for detection and screening • Then continue with full version
Current work II • Norms for CORE 65+ • Means and cut-off broadly comparable to <65 population • Means somewhat lower: • Clinical 1.49 65+ 1.87 <65 • Non-clinical 0.63 65+ 0.76 <65
Current work III • Teen-CORE • Several sites gathering clinical data • Jeremy Christie collecting normative data • “Kiddie-CORE” • still conceptual, design and methodological issues
Current work IV • Translated versions of CORE • Cantonese version performs well • Norwegian version being prepared • other European language versions needed
Current work V • Influencing the national agenda • Priority on severe and enduring mental illness • use of HoNOS and FACE • CORE for primary care?
Conclusions • Need both efficacy and effectiveness studies • Need to develop a national network to advance ‘effectiveness’ agenda within context of clinical governance (i.e., quality) • Need to adopt standard core outcome battery + referential measures (i.e., UK appropriate norms) • Progress to the adoption of ‘systems’ of service evaluation (e.g., CORE System/FACE System) • Address problem of attrition • Build national data base to inform clinical effectiveness