Download
1 / 12
200 likes | 616 Vues
İ. Çağatay Acuner M.D., Clinical Microbiologist , Associate Professor Department of Microbiology Faculty of Medicine , Yeditepe University , Istanbul cagatay.acuner@yeditepe.edu.tr. Nocardia (Aerobic Actinomycetes). Nocardia (Actinomycetes). Nocardia (Actinomycetes).

E N D
İ. Çağatay Acuner M.D., Clinical Microbiologist, Associate Professor Department of MicrobiologyFaculty of Medicine, Yeditepe University, Istanbul cagatay.acuner@yeditepe.edu.tr Nocardia (Aerobic Actinomycetes)
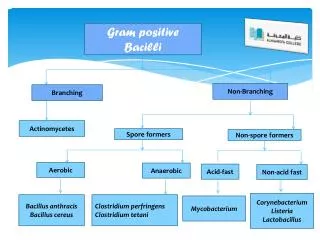
Nocardia (Actinomycetes) • Nocardiae are strict aerobic rods that form branched filamentous form in tissues and culture. • These filamentous forms resemble the hyphae formed by filamentous fungi (molds), and at one time Nocardia was thought to be a fungus. • However, the organisms have a gram-positive cell wall and other cellular structures that are characteristic of bacteria. • Most isolates stain poorly with the Gram stain and appear to be gram-negative with intracellular gram-positive beads • The reason for this staining property is that nocardiae have a cell-wall structure similar to that of mycobacteria; "weakly acid-fast"
Nocardia (Actinomycetes) • Cord factor is an important virulence factor that facilitates intracellular survival • Nocardia can grow on nonselective laboratory media ; growth is slow, requiring 3 to 5 days of incubation. (white to orange colonies withaerial hyphae) • Most infections are caused by a relatively few species • Identification at the genus level, with in vitro susceptibility testing, is sufficient for the management of most patients.
Nocardia (Actinomycetes) • Biology, Virulence, and Disease • Gram-positive, partially acid-fast, filamentous rods; cell wall with mycolic acid • Strict aerobe capable of growth on most nonselective bacteria, fungal, and mycobacterial media; however, prolonged incubation (7 days or more) may be required • Virulence associated with ability to avoid intracellular killing • Catalase and superoxide dismutase: inactivate toxic oxygen metabolites (e.g., hydrogen peroxide, superoxide) • Cord factor: prevents intracellular killing in phagocytes by interfering with fusion of phagosomes with lysosomes • Primary disease most commonly bronchopulmonary (e.g., cavitary disease) or primary cutaneous infections (e.g., mycetoma, lymphocutaneous infection, cellulitis, subcutaneous abscesses) • Dissemination most commonly to central nervous system (e.g., brain abscesses) or skin
Nocardia (Actinomycetes) • Epidemiology • Worldwide distribution in soil rich with organic matter • Exogenous infections acquired by inhalation (pulmonary) or traumatic introduction (cutaneous) • Opportunistic pathogen, causing disease most commonly in immunocompromised patients with T-cell deficiencies (transplant recipients, patients with malignancies, patients infected with the human immunodeficiency virus, patients receiving corticosteroids) • Diagnosis • Microscopy is sensitive and relatively specific when branching, partially acid-fast organisms are seen • Culture is slow, requiring incubation for up to 1 week; selective media (e.g., BCYE agar) may be required for isolating Nocardia in mixed cultures • Identification at the genus level can be made by the microscopic and macroscopic appearances (branching, weakly acid-fast rods forming colonies with aerial hyphae) • Identification at the species level requires genomic analysis for most isolates
Nocardia (Actinomycetes) • Treatment, Prevention, and Control • Infections are treated with antibiotics and proper wound care • Trimethoprim-sulfamethoxazole is used for localized infections; combination of antibiotics such as amikacin with a carbapenem or broad-spectrum cephalosporin is used for severe, progressive disease; treatment for 6 weeks or more • Exposure cannot be avoided, because nocardiae are ubiquitous
Nocardia (Actinomycetes) Acid-fast stain of Nocardia species in expectorated sputum. In contrast with the mycobacteria, members of the genus Nocardia do not uniformly retain the stain ("partially acid-fast"). Gram stain of Nocardia species in expectorated sputum. Note the delicate beaded filaments.
Nocardia (Actinomycetes) Aerial hyphae of Nocardia. Orange colonies of Nocardia
Nocardia (Actinomycetes) Nocardiosis: Clinical syndromes Bronchopulmonary disease: pulmonary disease with necrosis and abscess formation; dissemination to central nervous system or skin is common Mycetoma: chronic, destructive, progressive disease, generally of extremities, characterized by suppurative granulomas, progressive fibrosis and necrosis, and sinus tract formation Lymphocutaneous disease: primary infection or secondary spread to cutaneous site characterized by chronic granuloma formation and erythematous subcutaneous nodules, with eventual ulcer formation Cellulitis and subcutaneous abscesses: granulomatous ulcer formation with surrounding erythema but minimal or no involvement of the draining lymph nodes Brain abscess: chronic infection with fever, headache, and focal deficits related to the location of the slowly developing abscess(es)
Nocardia (Actinomycetes) Cutaneous lesion caused by Nocardia
Nocardia (Actinomycetes) Treatment, Prevention, and Control Nocardia infections are treated with the combination of antibiotics and appropriate surgical intervention. Trimethoprim-sulfamethoxazole is used most commonly to treat localized infections. In patients with severe, progressive disease, a combination of antibiotics is recommended, such as amikacin with a carbapenem (e.g., imipenem, meropenem) or broad-spectrum cephalosporin. In vitro susceptibility tests can be used to guide the selection of antibiotics. Because nocardiae can disseminate and produce significant disease, therapy should be extended for 6 weeks or more. Whereas the clinical response is favorable in patients with localized infections, the prognosis is poor for immunocompromised patients with disseminated disease. Nocardiae are ubiquitous, so it is impossible to avoid exposure to them. However, bronchopulmonary disease caused by nocardiae is uncommon in immunocompetent persons, and primary cutaneous infections can be prevented with proper wound care.