Download
1 / 23
230 likes | 440 Vues
Skeletal System. Bone. Bony skeleton 14% of adult weight 15% of newborn and 17% of young adult weight Also accounts for 97-98% of height, vertebral disk make up remaining height Functions of bone - Protection of vital organs - Support of body weight - storage for minerals

E N D
Bone • Bony skeleton 14% of adult weight 15% of newborn and 17% of young adult weight • Also accounts for 97-98% of height, vertebral disk make up remaining height • Functions of bone - Protection of vital organs - Support of body weight - storage for minerals - structural leverage for movement - bone marrow storage • Structure of bone, as well as stiffness and strength, allows it to meet functional demands or movement
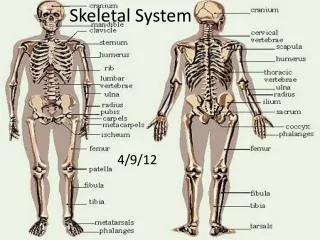
Terms • Osteoporosis – reduction in bone mass because of decreased formation of new bone or increased resorption • Osteopenia – organic or inorganic components fail to develop • Ostemalacia – abnormal mineralization of bone matrix because of calcium and phosphate deficiencies • epiphyseal plate-growth zone composed of hyaline cartilage • metaphysis-wider part of shaft of long bone • diaphysis-shaft of long bone formed by primary centers • epiphysis-ends of long bone formed by secondary centers
Skeletal System Development Prenatal Period • Development of bone via either intramembranous or endochondral ossification, begins in the embryonic period (3rd-8th gestational weeks) • Mesenchymal motels of bone appear in extremities, upper then lower at 5th week of gestation.
By 6th week mesenchymal cells have differentiated into chondroblasts which form cartilage model of long bones. • Primary ossification centers at 7th-8th week; by 12th week appear in most bones of the extremities. • Diaphyses fairly well ossified at birth, but epiphyses remain cartilaginous
Verterbral development begins in embryonic period; cartilage models of vertebrae are formed from mesenchymal cells located around the notochord. • By 7th-8th gestational week three ossification centers formed in the vertebrae model. • During early fetal period, most joints are formed. • In articular joints, mesenchyme differentiates into the joint capsule, ligaments, tendons and menisci. Depressions begin to form in the mesenchyme, resulting in formation of joint cavity and bursae. Once the joint is formed, intrauterine movement is important for ongoing joint development.
Bone formation occurs in diaphysis (central shaft of long bone) and growth cartilage (located at epiphyseal or growth plate, joint surface and apophyseal insertions of muscle tendon units • When epiphyseal plane becomes ossified long bones stop growing. Bones typically fuse during early adolescence with girls 2-3 yrs before boys
Infancy and Childhood • Particular concern is vulnerability of growth cartilage to trauma and overuse-disrupt blood and nutrient supply and permanent disturbances • Trauma from falls or excessive repetitive stress may result in a ligament tear or epiphyseal plate fracture. Peak incidence occurs at peak height velocity
Infancy and childhood are times of bone growth, modeling and remodeling. • Rapid growth in bone mineral density from 1-4 years and puberty • Bone mineral content increases more in 2-3 years surrounding peak height velocity than any other time (20-30% peak bone density and bone mineral content)
Children attain 50-60% of peak bone mass by puberty; 90% (boys) 95% (girls) before 20 years. • Before puberty boys and girls demonstrate linear increases in peak bone mineral density and content; after peak height velocity boys are higher because of increased testosterone levels. • Factors that contribute sex differences in bone mineral content and density are related to differences in bone shape and geometry, calcium intake and absorption, hormone production and physical activity levels.
Throughout infancy and early childhood, bone growth occurs rapidly affected by genetic makeup, nutrition, general health, and hormonal levels; rate and time of appearance in secondary ossification centers. • Physical activity beneficial, especially high-impact activity beneficial before peak height velocity; activity before puberty foster growth in muscle and bone mass. • Bone growth stimulated by weight bearing forces and mechanical pull of muscles. Activity places forces on growing bone which are important for optimal bone function.
Adolescence Structure, stiffness, strength > function • Aging losses-women 30, men 50 • Bone mass in third decade; men half of women • Appositional growth( laying down new bone on outer surface of the bone and is absorbed from the inner surface. Continues throughout life. In childhood and adolescence formation greater than absorption
Bone continues to grow and remodel in response to mechanical loading. Adolescent experiences increases in height and weight with growth of trunk in lower extremities. • Growth spurt in bone width seen in boys and girls up to 14. • Hormonal influences on growing bone change in puberty (sex hormones, androgens, and estrogen) influence bone growth and bone mineral acquisition. • High impact physical activity also increases site-specific bone mineral density in early puberty and adolescence.
Adulthood • After epiphyses closes, bones no longer lengthen • Throughout adulthood only bone remodeling occurs. Weight bearing and muscular contraction stimulate bone remodeling and increase bone density. • Adequate nutritional and calcium intake supports mineralization and remodeling.
Men and women attain maximal bone mass by late 20’s and 30 years • Bone formation and resorption remain balanced until 30-50 years (men) and 38-48 (women). After that bone loss is greater than bone replacement. In adult cortical bone loss begins in 4th decade and cancellous loss in third decade. • Women lose 1% of bone mass per year before menopause; 4-8 years after menopause bone loss is accelerated in women; then returns to 0.5-1% per year.
Men lose 0.5% of bone mass per year with decline in bone strength and risk for fractures and functional motor deficits. • Participation from childhood and adolescence show greater bone mass in adulthood; exercise increases muscle mass and generates force on bone. Appositional bone growth stimulated by weight bearing and strength training. • Fibrous cartilage in intervertebral disks change at 30 years (flatten, less resilient, loses ability to absorb water).
Older Adulthood • Skeletal system becomes more compromised • Limits mechanical loading of bone and circulation may be due to hormonal changes, dietary changes and decreased activity level. • Decreased estrogen levels are primarily responsible for loss of bone mineral density. • Maintaining physical activity and weight bearing, strength exercises maintain bone mineral density; functional loading helps balance bone formation and resorption.
Learning Activity • Growth cartilage in children is located at the epiphyseal plate; the joint surface, and apophyseal insertions. Damage to the growth cartilage may impair growth and development of affected bone