Download
1 / 50
500 likes | 612 Vues
Sameh W. Boktor, MD, MPH Medical Epidemiologist Pennsylvania Department of Health Harrisburg, Pennsylvania. Management of Patients with Chronic Hepatitis C: The Route to Safe and Effective Care. Disclosures.

E N D
Sameh W. Boktor, MD, MPH Medical Epidemiologist Pennsylvania Department of Health Harrisburg, Pennsylvania Management of Patients with Chronic Hepatitis C: The Route to Safe and Effective Care
Disclosures • Sameh Boktor, MD, has no financial interests/relationships or affiliations in relation to this activity. • This activity was independently peer-reviewed by CME Peer Review. Neither of the independent reviewers had relevant financial relationships to disclose. Off-label and/or investigational use of pharmaceuticals may be discussed in the presentation. This disclosure is to ensure participants in the activity may formulate their own judgments regarding the presentation.
Learning Objectives • Evaluate the most recent clinical guidelines to improve screening for and diagnosis of infection with hepatitis C virus (HCV) • Optimize current evidence-based components of chronic HCV therapy based on patient status, HCV genotype, comorbidities, and concomitant therapies • Integrate methods to minimize toxicities and adequately manage treatment-related adverse effects • Evaluate the utility of investigational therapies for the treatment of HCV
Hepatitis C: Burden of Disease in the U.S. • About 5.2 million infected individuals in the United States currently (~2% of the population) • Leading cause for liver transplant and liver cancer • Number of patients with morbidity and mortality from chronic HCV increasing • Approximately 1.76 million persons with untreated chronic HCV infection will develop cirrhosis over the next 40 to 50 years • The projected incidence peak of end-stage liver disease will occur in 2030, with about 38,600 cases per year • Transplants are expected to peak in 2032 to 2033 at level of 3200 HCV-related transplants per year Rein et al. Dig Liver Dis 2011;43:66-72. Zalesak et al. PLOS ONE 2013;8(5):e63959.
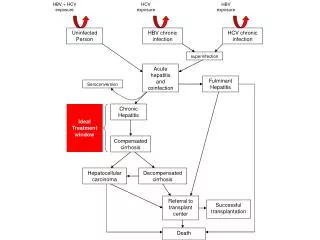
Chronic HCV Infection May Lead to Chronic Liver Disease or Liver Cancer In 1-4% patients, cancer of the liver will develop Over time, fibrosis can lead to severe scarring or cirrhosis in 10-20% patients Chronic hepatitis occurs in 75-85% of infected individuals and can lead to fibrous scar within the liver • Decompensated cirrhosis (5-year survival rate of 50%): • Ascites • Jaundice • Hepatic encephalopathy • Edema • Renal failure • Variceal bleeding • Spontaneous bacterial peritonitis Davis et al. Gastroenterology 2009;138(2):513-521. Huffman et al. JABFM 2014;27(2):284-291.
Extrahepatic Manifestations of Chronic Hepatitis C • Hematologic disorders • Essential mixed cryoglobulinemia • Monoclonal gammopathies • Lymphoma (non-Hodgkin’s B cell) • Anemia, thrombocytopenia, coagulopathy • Autoimmune disorders • Autoantibodies • Autoimmune hepatitis • Thyroid disease • Cardiac • Myocarditis • Cardiomyopathy • Dermatologic • Porphyria cutaneatarda • Leukocytoclastic vasculitis • Lichen planus • Rheumatologic • Arthritis • Renal • Membranoproliferative glomerulonephritis • Membranous nephropathy • Renal failure • Endocrine • Diabetes mellitus Cacoub et al. The GERMIVIC 2000;79:47.
Gaps in Hepatitis C Screening and Treatment • National survey of PCPs revealed 73% of respondents reported seeing five or fewer patients with HCV per year, 44% reported no experience with HCV treatment, and only 59% actually screened for HCV • Due to lack of awareness of the current advances in HCV, only ~50% of patients with HCV are referred for subspecialty evaluation Mitchell et al. Hepatology 2010;51:729-33. Shehab et al. Journal of viral hepatitis 2001;8:377-83.
Identifying Patients With Chronic Hepatitis C • An estimated 40 to 85% of persons infected with HCV are unaware of their HCV infection status • One study reported that amongst HCV-infected injection drug users who were 15 to 30 years old, 72% were unaware of their HCV infection status • NHANES study conducted from 2001 through 2008 found that 50.3% of persons infected with HCV were unaware of their status • In a study involving persons with access to medical care in four private health care organizations during the years 2006 to 2008, an estimated 43% were unaware of their HCV infection Armstrong et al. Ann Intern Med.2006;144:705-14. Denniston MM et al. Hepatology2012;55:1652-61. Denniston MM et al.Ann Intern Med.2014;160:293-300.
Hepatitis C Testing in the U.S. 2012 Kaiser study including HI, OR, MI, PA sites Spradling PR et al. CID 2012;55(8):1047-1055.
Who Should be Tested: USPSTF Grade B Recommendations • Everyone born from 1945-1965 (one-time) • Past or present injection drug use • Sex with an IDU; other high risk sex • Blood transfusion prior to 1992 • Persons with hemophilia • Long-term hemodialysis • Born to an HCV-infected mother • Incarceration • Intranasal drug use • Unregulated tattoo • Occupational percutaneous exposure • Surgery prior to universal precautions Smith et al. Ann Intern Med 2012;157:817-822. Moyer et al. Ann Intern Medepub 25 June 2013.
HCV Screening Interval • Persons in the birth cohort and those who are at risk because of potential exposure before universal blood screening and are not otherwise at increased risk need only be screened once. • Persons with continued risk for HCV infection (injection drug users) should be screened periodically. • The USPSTF found no evidence about how often screening should occur in persons who continue to be at risk for new HCV infection. http://www.uspreventiveservicestaskforce.org/uspstf12/hepc/hepcfinalrs.htm
HCV Testing Algorithm Rapid or lab-conducted assay HCV ANTIBODY TEST NON-REACTIVE REACTIVE NOT DETECTED HCV RNA TEST * STOP RESOLVED INFECTION STOP FALSE + TEST DETECTED * For persons who might have been exposed to HCV within the past 6 months, testing for HCV RNA or follow-up testing for HCV antibody should be performed. For persons who are immunocompromised, testing for HCV RNA should be performed. FURTHER ANTIBODY TESTING AS INDICATED CURRENT HCV INFECTION Adapted from Centers for Disease Control and Prevention (CDC), 2013.
FDA-approved Commercially Available HCV Antibody Tests Anti-HCV = HCV antibody; EIA = enzyme immunoassay; CIA = chemiluminescentimmunoassay; MEIA = microparticle enzyme immunoassay; CMIA = chemiluminescentmicroparticle immunoassay GhanyMG et al. Hepatology. 2009. 49: 1335-74.
Confirmatory Testing for HCV Infection • Molecular Testing (HCV quantitative test) • Nucleic acid testing • Not intended for diagnosis of acute hepatitis C • Abbott Real Time HCV • Detection range 12IUml-100 million IU/ml • Roche COBAS Taq Man HCV • Detection range 43IU/ml-69 million IU/ml • Genotypic Testing • Trugene 5NC HCV Genotyping kit (Siemens Healthcare Diagnostics Division, Tarrytown, NY) • Versant HCV Genotyping Assay 2.0 (Siemens Healthcare Diagnostics Division, Tarrytown, NY) • INNO-LiPaHCV II, (Innogenetics, Ghent, Belgium) GhanyMG et al. Hepatology. 2009. 49: 1335-74.
HCV Genotype Distribution in the United States 1.2% 0.5% 9.6% 11.3% 60.3% 16.7% Data reported on https://www.labcorp.com
Next Steps in Evaluation of HCV Infected Individuals • Abstinence from alcohol and, when appropriate, interventions to facilitate cessation of alcohol consumption • Evaluation for other conditions that may accelerate liver fibrosis, including HBV and HIV infections • Evaluation for advanced fibrosis is recommended using liver biopsy, imaging, or non-invasive markers to facilitate an appropriate decision regarding HCV treatment strategy and to determine the need for initiating additional screening measures (hepatocellular carcinoma [HCC] screening, variceal screening) • Vaccination against hepatitis A and hepatitis B • Education on how to avoid HCV transmission to others • Evaluation by a practitioner who is prepared to provide comprehensive management including consideration of antiviral therapy
Recommendations for Preventing Transmission • Avoid sharing toothbrushes, dental and shaving equipment and cover any bleeding wound. • Avoid obtaining tattoos and piercings at non-reputable, unlicensed facilities that do not sterilize equipment. • Avoid donating blood and discuss serostatus prior to donation of body organs, other tissue or semen. • Use barrier protection for MSM with HIV infection and those with multiple sex partners. Others with HCV infection should be counseled that risk of sexual transmission is low and may not warrant barrier protection. http://www.hcvguidelines.org
Recommendations for Preventing Transmission • Decontaminate household surfaces and implements with visible blood from an HCV-infected person with dilution of 1 part household bleach:9 parts water. Wear gloves for cleaning. • For illicit drug users, stop using and enter substance abuse treatment. If drug use is continued, then avoid reusing or sharing syringes, needles, water, cotton and other drug preparation equipment. New sterile syringes, filters, and disinfected cookers should be used. Needles and syringes should be disposed of in safe, puncture-proof containers. http://www.hcvguidelines.org
Eligibility Criteria for Chronic HCV Treatment • Age 18 years or older • Detectable serum HCV RNA • Liver biopsy with chronic hepatitis and significant fibrosis (historic criteria, not currently mandated) • Compensated liver disease • Acceptable hematologic and biochemical indices • Willing to be treated and conform to treatment requirements • No contraindications to treatment • Need to consider additional factors such as: alcohol use, drug use, chronic kidney disease, prior liver transplant
Non-invasive Biomarkers of Fibrosis Baranova et al. BMJ Gastro 2011;11:91.
Contraindications to Treatment with Peg-IFN • Major uncontrolled depression • Solid organ transplant (e.g., kidney, heart or lung) • Autoimmune hepatitis or other autoimmune condition • Untreated thyroid disease • Pregnant or unwilling to practice effective birth control • Severe accompanying diseases, such as very high blood pressure, heart failure, significant coronary disease, poorly controlled diabetes and chronic obstructive disease/emphysema • A parent of children younger than 2 years old • Known allergies to the drugs used to treat HCV
Evolution of Hepatitis C Treatment Ribavirin Telapravir and boceprivir Potential approval of other DAAs Interferon Proof of concept for DAAs (PI) 1990 2005 2014 2000 2010 2011 2012 2013 2015+ Supression of HCV with DAA combination (PI + NI) Pegylatedinterferons FDA approval of simeprivir and sofosbuvir with IFN IFN-free therapy
Categories of Therapy Response Modified from: Ghany MG ,et al. Hepatology 2009;49:1335-74. *Developed primarily for response-guided therapy.
Goal of Treatment • HCV RNA negativity 6 months post-treatment • Predicts 99% chance of remaining RNA negative long-term and considered a cure Sustained viral response (SVR)
Chronic HCV Therapy (Genotype 1): Advances in Raising Cure Rates >90% ~70% 44% 35% 16% Schaefer EA et al. Gastroenterology. 2012;142:1340-1350. Ghany MG et al. Hepatology. 2009;49:1335-1374. Ghany MG et al. Hepatology. 2011;54:1433-1444.
Targets for Direct-Acting Antiviral Agents (DAAs) • Prevent viral entry • Polyclonal and monoclonal antibodies • Prevent translation of viral RNA • NS3/4 protease inhibitors • Inhibit HCV-RNA polymerase • Nucleoside analogue NS5B poly. inhib • Non-nucleoside analogue NS5B poly inhib • Replication complex inhibitor • Cyclophilin B inhibitors • Viral assembly/release • Glucosidase inhibitor Pereira et al. Nat Rev GastroenterolHepatol. 2009;6:403-411. http://trialx.com
Selected Characteristics for Direct Acting Agents for Chronic Hepatitis C Infection Schaefer et al. Gastroenterology 2012;142:1340-1350.
Simeprivir • NS3/4A protease inhibitor FDA-approved November 2013 • In combination with PR in G1 patients, can achieve overall SVR rate 75-85% • Contraindications: • Monotherapy • Substances that are moderate or strong inducers or inhibitors of cytochrome P450 3A (CYP3A) • Pregnancy or a male whose female partner is pregnant • No dose adjustment needed for in any type of renal impairment or mild hepatic impairment • Adverse reactions: rash, photosensitivity, pruritus, nausea, myalgia, dyspnea • Use not indicated in HIV/HCV co-infection, hepatocellular cancer, liver transplant Jacobson I et al. J Hepatol. 2013;58(suppl 1):S574. Abstract 1425. Manns M et al. J Hepatol. 2013;58(suppl 1):S568. Abstract 1413.
Simeprivir + PR • Need to check Q80K polymorphism prior to treatment • Simeprivir150mg + weight-based PR • Treatment-naïve and prior relapsers (including cirrhotics): • SIM + PR x 12 weeks + additional PR x 12 weeks • Total duration of therapy = 24 weeks • Partial and null responders (including cirrhotics): • SIM + PR x 12 weeks + additional PR x 36 weeks • Total duration of therapy = 48 weeks • Stop all treatment if: HCV RNA ≥25 IU/mL at either week 4, 12, or 24
Simeprivir + PR: SVR Rates • Pooled QUEST 1 and QUEST 2 • SVR in treatment-naïve only, rates are lower in prior relapsers, partial responders and null responders Jacobson I, et al. J Hepatol. 2013;58(suppl 1):S574. Abstract 1425. Manns M, et al. J Hepatol. 2013;58(suppl 1):S568. Abstract 1413.
Sofosbuvir • Nucleotide analog NS5B polymerase inhibitor • FDA-approved December 2013 • Contraindications: • Monotherapy • P-gp inducers (St. John’s Wort, rifampin) • Pregnancy or a male patient whose female partner is pregnant • No dose can be recommended in severe renal disease or end-stage liver disease • Adverse reactions: headache, fatigue, nausea, insomnia, anemia • May be used in HIV/HCV co-infection, hepatocellular cancer, those awaiting liver transplant Lawitzet al. J Hepatol. 2013;58(suppl 1):S567. Abstract 1411. Lawitzet al. N Engl J Med. 2013;368:1878-1887.
Sofosbuvir + PR • FDA-approved for combination with PR (pegIFN + RBV) for 12 weeks in genotypes 1, 4 • Off-label use in genotypes 5, 6 • Can achieve overall SVR > 90% • To be used in treatment-naïve patients only • No resistance detected, 1 relapse in patient who discontinued therapy • Well-tolerated no additive effects of addition of sofosbuvir to PR LawitzE, et al. J Hepatol. 2013;58(suppl 1):S567. Abstract 1411. LawitzE, et al. N Engl J Med. 2013;368:1878-1887.
SVR12 Rates by Subgroups: NEUTRINO Study Cirrhotic IL-28B *P<0.001 vs historical SVR rate 60% LawitzE, et al. J Hepatol. 2013;58(suppl 1):S567. Abstract 1411. LawitzE, et al. N Engl J Med. 2013;368:1878-1887.
Sofosbuvir + Ribavirin • FDA-approved for genotypes 2, 3, 4 • Sofosbuvir 400mg + weight-based RBV • Genotype 2: 12 weeks • Genotype 3: 24 weeks • Genotype 4: 24 weeks • Treatment-naïve and experienced patients • Alternate therapy for interferon-intolerant G1 patients Gane E et al. J Hepatol. 2013;58(suppl 1);S3. Abstract 5. LawitzE et al. N Engl J Med. 2013;368:1878-1887. Nelson ER, et al. J Hepatol. 2013;58(suppl 1):S3-S4. Abstract 6. Jacobson IM, et al. N Engl J Med. 2013;368;1867-1877. Jacobson IM, et a. J Hepatol. 2013;58 (suppl 1);S28. Abstract 61.
SOF + RBV: SVR12 Rates by Subgroup Gane E et al. J Hepatol. 2013;58(suppl 1);S3. Abstract 5. LawitzE et al. N Engl J Med. 2013;368:1878-1887. Nelson ER, et al. J Hepatol. 2013;58(suppl 1):S3-S4. Abstract 6. Jacobson IM, et al. N Engl J Med. 2013;368;1867-1877. Jacobson IM, et a. J Hepatol. 2013;58 (suppl 1);S28. Abstract 61.
Dose Adjustment: Ribavirin Ribavirin Dose Modification Guideline for Coadministration with Sofosbuvir
Sofosbuvir + RBV: HCV/HIV Coinfection • Sofosbuvir 400mg daily + weight-based RBV daily x 12 weeks • PHOTON-1 Study • Treatment naïve genotype 1-3 • Included compensated cirrhotics • Stable HIV disease • ART was FTC/TDF plus either efavirenz (34%), atazanavir/r (17%), darunavir/r (18%), raltegravir (16%), rilpivirine (6%) • SVR 76%(genotype 1, 24 weeks therapy), 88%(genotype 2, 12 weeks), 67%(genotype 3, 12 weeks) Sulkowski MS et al. Hepatology. 2013;58(suppl 1):313A-314. Abstract 212.
HCV RNA Monitoring: Sofosbuvir-based Regimens • Monitoring does not affect treatment course • 99% achieved undetectable HCV RNA at week 4 • 8% treatment failure due to relapse • No official recommendation to check HCV RNA until after therapy • Most providers check RNA level week 4 to document compliance and at end of treatment (week 12 or 24)
Effect of Illicit Drugs, Alcohol, and Marijuana on Treatment • Illicit drug use • No difference in SVR between users and non-users • Studies with sofosbuvir only included those on opiate replacement therapy and there was no difference in SVR • Decision to treat on individual basis • Alcohol use • Higher viral loads in alcohol-users (blunts immune response) • Rate and severity of liver damage • Risk for hepatocellular cancer • Cessation leads to SVR rate of non-drinkers • Alcohol treatment program or sober x 6 months • Marijuana use • Possible hepatic steatosis/fibrosis in daily users
DAA + PR in Late-Stage Clinical Development • STARTVerso1 Trial: • Phase 3, treatment-naïve, genotype 1 • Faldaprevir 120mg qd or 240mg qd + PR x 12 weeks + PR versus Faldaprevir + PR for additional 12 weeks • Overall SVR12 rates: • 79% (Faldaprevir 120mg + PR) • 80% (Faldaprevir 240mg + PR) • 52% (PR) Ferenci P et al. J Hepatol. 2013:58(suppl 1):S569-S570. Abstract 1416.
Multiple DAA + PR in Late Stage Clinical Development • MATTERHORN Study: Danoprevir + Mericitabine + PR in G1 • Quad treatment SVR12 86% (partial responders) and 84%(null responders) • Virologic breakthrough related to danoprevir resistance • Regimens were safe and well-tolerated • Study 011: Daclatasvir + Asunaprevir +/- PR in G1 • SVR12 90% and 97% in quad arms • No discontinuations • Adverse effects included headache, diarrhea, fatigue, insomnia Feld JJ et al. Hepatology. 2012;56(suppl 4):231A-232A. Abstract 81.
Sofosbuvir + Ledipasvir: Treatment-Naïve Patients • FDA APPROVAL FOR THIS COMBINATION FILED FEB. 10, 2014 • ION-1 Trial: Phase 3, N=865,N Engl J Med 2014; 370:1483-149 • Ledipasvir also an NS5A inhibitor • Combination tablet of Ledipasvir 90 mg/Sofosbuvir 400 mg once daily + RBV bid • Combo tablet 12 weeks – SVR 99% • Combo tablet + RBV 12 weeks – SVR 97% • Combo tablet 24 weeks – SVR 98% • Combo tablet + RBV 24 weeks – SVR 99% • 3 had virologic failure: 1 suspected non-adherence, 2 relapsed • No benefit with Ribavirin
Sofosbuvir + Ledipasvir: Treatment-Experienced Patients • ION-2 Trial: Phase 3, patients previously treated with PR +/- protease inhibitor, N=440, N Engl J Med 2014; 370:1483-1493 • Combination tablet of Ledipasvir 90 mg/Sofosbuvir 400 mg once daily + RBV bid • SVR measured at 12 weeks post-treatment completion • Combo tablet 12 weeks – SVR 94% • Combo tablet + RBV 12 weeks – SVR 96% • Combo tablet 24 weeks – SVR 99% • Combo tablet + RBV 24 weeks – SVR 99% • No drop-outs for side effects • No significant benefit with RBV
Sofosbuvir + Simeprivir ± RBV • COSMOS study: Open-label, G1, prior PR null responder, non-cirrhotics and cirrhotics • SIM + SOF qd vs SIM + SOF + RBV qd x 12 or 24 weeks • Interim results Jacobson IM et al. Hepatology. 2013;58(suppl 1):73A. Abstract LB-3.
ABT-450/R/ABT-267 + ABT-333 + RBV: Treatment-experienced G1 • SAPPHIRE II: Phase 3, placebo-controlled, 12 week regimen, non-cirrhotic, N=394 • ABT-450 150mg + ritonavir 100mg + ombitasvir 25mg + dasabuvir 250mg bid + RBV 1000-1200mg • Overall SVR12 – 96% • Relapsers SVR12 – 95% • Partial responders SVR12 – 100% • Null responders SVR12- 95% • 2.4% relapse rate Zeuzem S et al. EASL abstract O1. J Hepatology 2014;60(suppl 1):S1.
Conclusions • It is important to recognize patients who should be screened for hepatitis C infection • There are many factors that contribute to treatment decisions • The decision to treat depends on the patient’s risk for progression of disease and anticipated efficacy of the drug combination • SVR decreases liver-related complications and all-cause mortality • Treatment options are rapidly changing • Traditional prognostic factors becoming obsolete • Not all patients need to be urgently treated
Conclusions Cont’d • Results from phase 3 trials for all-oral agents are excellent, with well tolerated regimens and high SVR rates • Interferon-free regimens with high SVR rates are possible in a variety of populations, including difficult-to-treat patients • Ribavirin and IL28B status important for DAA + PR regimens • Further study needed in: • Cirrhosis, HIV coinfection, liver transplant recipients, genotype 4, patients who fail therapy with newer DAA’s
Resources for Patients • www.hepmag.com • www.AASLD.org/patients • www.cdc.gov/hepatitis/C • www.hepeducation.org • www.hepc.liverfoundation.org • www.hepatitis.va.gov/HEPATITIS