Download
1 / 19
200 likes | 380 Vues
BRACHIAL PLEXUS INJURY IN NEONATES LOURDES ASIAIN February 2005. BACKGROUND. 1764 Obstetrical brachial palsy described by Smellie.

E N D
BRACHIAL PLEXUS INJURY IN NEONATES LOURDES ASIAIN February 2005
BACKGROUND • 1764 Obstetrical brachial palsy described by Smellie. • 1874 Wilhelm H. Erb described brachial plexus paralysis in adults which involved the upper roots and described certain types of “delivery paralysis”. He credited Duchenne for describing the brachial palsy following delivery in affected newborns. • 1885 Augusta Klumpke first described the clinical picture resulting from injury to lower roots.
EPIDEMIOLOGY Incidence of brachial plexus palsy is reported to affect 0.5 to 1.9 per 1000 live births (Bar et al 2001) 90% Erb palsy Most common on the right side because the most common delivery presentation is left occiput anterior vertex. Associated with: pre and gestational diabetes older maternal age increased BW, LGA Newborns with BP injuries have a higher incidence of low Apgar scores of less than 7 at 1 and 5 mins and of asphyxia than matched controls
EPIDEMIOLOGY Brachial plexus palsy occurs in 26% of cases of shoulder Dystocia Both Shoulder dystocia and brachial plexus palsy are more common in LGA babies and Infants of diabetic mothers Infants of diabetic mothers have a higher incidence of permanent impairment In infants of diabetic mothers, the macrosomic process affects the trunk but not the head (large biacromial diameter) The head shoulder disproportion is difficult to predict in Utero.
EPIDEMIOLOGY Clavicular fractures are often associated with shoulder dystocia , but the incidence of brachial palsy in these Cases is only 11%. Clavicular fracture =more mobility of shoulder Not always associated with difficult delivery (Intrauterine Maladaption palsy). Cases of in utero origin supported by EMG findings if denervation at birth.
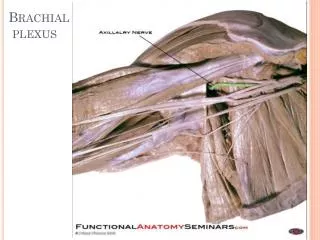
Brachial plexus is comprised of a group of nerves arising form the nerve roots C5-T1. The uppper (C5-C6) roots innervate the deltoid, spinati,biceps, brachioradialis, biceps supinator and flexor muscles of the forearm. The lower roots (C7-T1) innervate the intrinsic muscles of the hand. The phrenic nerve, arising from C3-C5 can be involved resulting in ipsilateral diaphragmatic paralysis causing a decrease in thoracic space, tidal volume and vital capacity. Involvement of the sympathetic nerves from T1 that give rise to the sup cervical symp ganglion can result in Horner Synd.
HORNER SYNDROME Ptosis Miosis and anhydrosis
Stretch, tear, compression or avulsion of the nerves usually after forceful lateral deviation of the head from the shoulders during delivery. Recent studies suggest intrinsic forces (uterine contractions). PATHOGENESIS
Clinical Manifestations: Asymmetric Moro reflex Erb palsy caused by the disruption of the upper brachial plexus. Posture of adduction and inward rotation at the shoulder with extension and pronation at the elbow and flexion of the fingers = WAITER’S TIP Klumpke= absent grasp reflex of the hand
Clinical Manifestations If phrenic nerve is involved, as mentioned earlier respiratory distress may be present.
DIFFERENTIAL DIAGNOSIS Cervical Injury Cervical Spine injury Dislocation of upper extremity/fractures of upper extremity Intrauterine maladaptation palsy The physical findings of BP palsy are so unique so it is difficult to mistaken if for other diagnosis.
DIAGNOSTIC WORKUP Evaluation can be undertaken by multiple modes of Imaging. EMG MRI Chest X ray Real time UltraSonography
MANAGEMENT The majority of patients with brachial plexus palsy Dx at birth will recover from neurologic deficit. Those who do not recover during 3-6month period will Require surgical intervention. 1-2 week rest of affected limb Early referral to upper extremity clinic and PT Caregivers should be instructed on how to handle baby: No traction of affected arm, no pressure under axila. Baby to be carried in football hold
MANAGEMENT Surgical • Exploration • Neurolysis • Excision of scar tissue • Nerve grafting (local end to end anastomosis or remote • nerve transplant) • Surgical plication in case of diaphragmatic involvement • Special considerations in post surgical care: • Edema of neck and compromise of airway • Injury to vagal and laryngeal nerves • Risk for meningitis
PROGNOSIS Study by Noetzel et al (2001) followed 80 patients with BP injury who did not recover by 2 weeks of age. Used the BMRC scales for evaluating muscle strength and found: Complete recovery in 66% Mild impairment in 11% Moderate weakness was seen in 9% Severe weakness in 14% When associated with phrenic nerve palsy and diaphragmatic paralysis, there is more likelihood of need for surgery for recovery.
REFERENCES • Brachial plexus palsy in neonates John B Cahil, Medlink Brachial plexus injury and obstetrical risk factors. Int J Gynecol Obst 2001;73 (1) 21-5 Brachial plexus injuries, emedicine Aug 2004