Download
1 / 24
270 likes | 454 Vues
Asymptomatic carotid stenosis Identification of the high-risk patient. Richard Bulbulia Consultant Vascular Surgeon CTSU, University of Oxford And Cheltenham General Hospital. Projected Rise in Stroke Mortality Worldwide to 2030.

E N D
Asymptomatic carotid stenosis Identification of the high-risk patient Richard Bulbulia Consultant Vascular Surgeon CTSU, University of Oxford And Cheltenham General Hospital
Average annual risk rates of Ipsilateral stroke in patients with at least 50% asymptomatic carotid stenosis OXVASC study, Stroke 2010;41:e11-e17.
Despite intensive statin therapy residual cardiovascular risk remains high • SEARCH trial: a trial comparing intensive vs. moderate LDL-lowering (80 mg simvastatin vs. 20 mg) • 6031 post-MI patients allocated simvastatin 80mg daily for 7 years • Annual vascular death rate: 1.4% • Annual major vascular event rate: 3.6% 10-year risk of major vascular event over 30% and risk of death almost 15%
Residual Stroke Risk • 1.0% yearly post-procedural stroke risk in ACST 10 year follow-up amongst those allocated immediate CEA • Stroke rates of 1.0% per year seen in the long-term follow-up of HPS (17,000 high-risk patients receiving good LDL-lowering therapy)
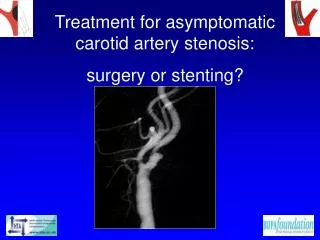
What is the net benefit of carotid intervention? Procedural risk Long-term efficacy Natural history of asymptomatic stenosis
Degree of stenosis and stroke risk ACST 10-year Results: First non-perioperative stroke by % ipsilateralstenosis
Contralateral occlusion and stroke risk ACST 10-year Results: First non-perioperative stroke by contralateteral status
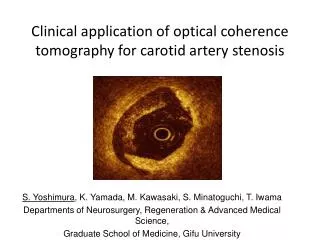
TCD micro-emboli and stroke risk Source: The Lancet Neurology 2010; 9:663-671 (DOI:10.1016/S1474-4422(10)70120-4)
Importance of previous brain infarctsin patients with asymptomatic carotid stenosis and the impact of surgery from the Asymptomatic Carotid Surgery Trial (ACST-1) trial Jonathan Y. Streifler MD, Anne G. den Hartog MD, Samuel Pan, Hongchao Pan PhD, Richard Bulbulia MD, Dafydd J. Thomas MD, Alison Halliday MD on behalf of the ACST-1 trial collaborators ISC Hawaii Disclosure: None
Silent brain infarcts • MRI-defined silent brain infarcts (SBI’s) are detected in 20% of healthy elderly people • SBI’s are detected in up to 50% of patients in selected series. • Although silent infarcts, by definition, lack clinically overt stroke-like symptoms, they are associated with subtle deficits in physical and cognitive function that commonly go unnoticed. Vermeer SE et al, Silent brain infarcts: a systematic review. Lancet Neurol 2007;6:611
Methods • ACST-1 included 3120 patients • Baseline brain imaging was identified in 2333 patients and these were divided into 2 groups: 1. Group 1: 1331 patients with prior brain infarcts (i.e. radiological evidence of an asymptomatic infarct or prior ischemic symptoms >6 months prior to randomization). Only 31 had normal brain imaging. 2. Group 2: 1002 patients with normal imaging and no prior symptoms. All participants were randomly allocated either immediate or deferred CEA.
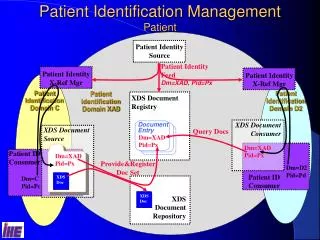
PBI No PBI
Number of the first episode of stroke events observed in group 1 and 2 * From Cox proportional hazards model, adjusting all other baseline variables listed in table 1
Cause-specific numbers of deaths, separated for group 1 and group 2 * From Cox proportional hazards model, adjusting all other baseline variables listed in table 1
Conclusions In ACST 1… Prior brain infarcts were common (>1/3rd) Associated with increased risk of carotid territory stroke May help identify a population in whom carotid intervention is particularly worthwhile