Download
1 / 1
10 likes | 134 Vues
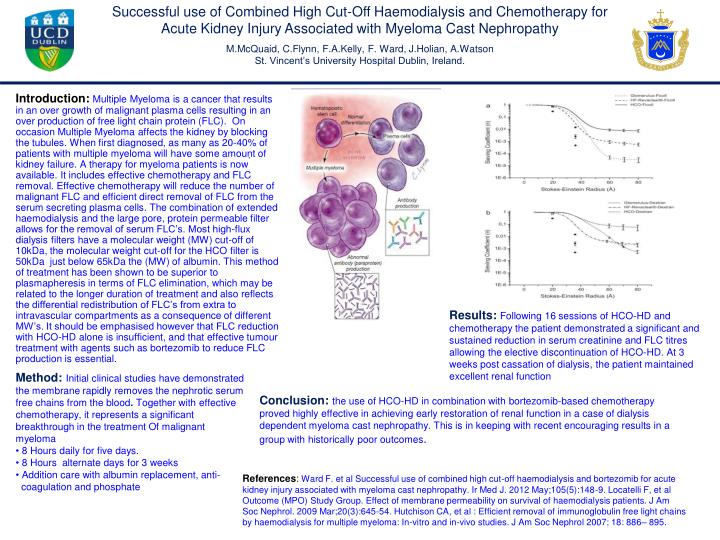
Successful use of Combined High Cut-Off Haemodialysis and Chemotherapy for Acute Kidney Injury Associated with Myeloma Cast Nephropathy M.McQuaid, C.Flynn, F.A.Kelly, F. Ward, J.Holian, A.Watson St. Vincent’s University Hospital Dublin, Ireland.

E N D
Successful use of Combined High Cut-Off Haemodialysis and Chemotherapy for Acute Kidney Injury Associated with Myeloma Cast Nephropathy M.McQuaid, C.Flynn, F.A.Kelly, F. Ward, J.Holian, A.Watson St. Vincent’s University Hospital Dublin, Ireland. Introduction:Multiple Myeloma is a cancer that results in an over growth of malignant plasma cells resulting in an over production of free light chain protein (FLC). On occasion Multiple Myeloma affects the kidney by blocking the tubules. When first diagnosed, as many as 20-40% of patients with multiple myeloma will have some amount of kidney failure. A therapy for myeloma patients is now available. It includes effective chemotherapy and FLC removal. Effective chemotherapy will reduce the number of malignant FLC and efficient direct removal of FLC from the serum secreting plasma cells. The combination of extended haemodialysis and the large pore, protein permeable filter allows for the removal of serum FLC’s. Most high-flux dialysis filters have a molecular weight (MW) cut-off of 10kDa, the molecular weight cut-off for the HCO filter is 50kDa just below 65kDa the (MW) of albumin. This method of treatment has been shown to be superior to plasmapheresis in terms of FLC elimination, which may be related to the longer duration of treatment and also reflects the differential redistribution of FLC’s from extra to intravascular compartments as a consequence of different MW’s. It should be emphasised however that FLC reduction with HCO-HD alone is insufficient, and that effective tumour treatment with agents such as bortezomib to reduce FLC production is essential. . Figure 2 Results: Following 16 sessions of HCO-HD and chemotherapy the patient demonstrated a significant and sustained reduction in serum creatinine and FLC titres allowing the elective discontinuation of HCO-HD. At 3 weeks post cassation of dialysis, the patient maintained excellent renal function • Method: Initial clinical studies have demonstrated the membrane rapidly removes the nephrotic serum free chains from the blood. Together with effective chemotherapy, it represents a significant breakthrough in the treatment Of malignant myeloma • 8 Hours daily for five days. • 8 Hours alternate days for 3 weeks • Addition care with albumin replacement, anti- • coagulation and phosphate Conclusion: the use of HCO-HD in combination with bortezomib-based chemotherapy proved highly effective in achieving early restoration of renal function in a case of dialysis dependent myeloma cast nephropathy. This is in keeping with recent encouraging results in a group with historically poor outcomes. References:Ward F. et al Successful use of combined high cut-off haemodialysis and bortezomib for acute kidney injury associated with myeloma cast nephropathy. Ir Med J. 2012 May;105(5):148-9. Locatelli F, et al Outcome (MPO) Study Group. Effect of membrane permeability on survival of haemodialysis patients. J Am Soc Nephrol. 2009 Mar;20(3):645-54. Hutchison CA, et al : Efficient removal of immunoglobulin free light chains by haemodialysis for multiple myeloma: In-vitro and in-vivo studies. J Am Soc Nephrol 2007; 18: 886– 895.